
![]()
Funtabulously Frivolous Friday Five 283
Just when you thought your brain could unwind on a Friday, you realise that it would rather be challenged with some good old fashioned medical trivia FFFF, introducing the Funtabulously Frivolous Friday Five 283
Question 1
What is the Windkessel effect?
Reveal the funtabulous answer
During systole the elastic fibers of the aorta allow the aorta to stretch and expand, during diastole retraction of the elastic fibers of the aorta help propel blood forward. The effect of this elasticity is the Windkessel effect, which results in a smoothing of the pulsatile flow through the aorta and a decrease in pulse pressure.
Windkessel in German literally means ‘air chamber’.
Question 2
Which eminent London surgeon did the Lancet editorial team berate in 1828, and why?
This surgical cock sparrow has been hopping and fluttering about lately at a great rate, and chirping away at the height of its lungs to its own complete satisfaction…Some people are so stupid, that they ought not to be trusted at large without a keeper; they will run their heads against walls or posts, if any are to be met with.
Reveal the funtabulous answer
Henry Earle (1789 – 1838)
Most commonly remembered (or rather forgotten…) for his description of fracture-dislocation of the ankle with avulsion of the posterior edge of the tibia. Initially described as Earle triangle (Lauge, 1948) but now referred to as Volkmann triangle
Earle designed a fracture bed for the conservative management of neck of femur fractures first published in Practical observations in surgery in 1823 then re-designed and reviewed in the Lancet 1824. The device provided comfort for the patient; allowed treatment of the femoral neck fracture in semiflexion; and allow fractures of the neck of the thigh-bone to unite without surgical intervention. This caused a war of words with Sir Astley Cooper…and ultimately the Lancet
The ‘Lancet,’ didn’t much care for Earle. They made many indecent attacks on him referring to his teachings the ‘chirrupings of a cock-sparrow, ’ (for his diminutive stature). Quite a series of tirades from the editorial staff of the illustrious journal… [Lancet 1828: 597-600; Lancet 1829: 255-258]
Question 3
Patients with which disorder, have the strongest HLA association, should not be startled during dinner time?
Reveal the funtabulous answer
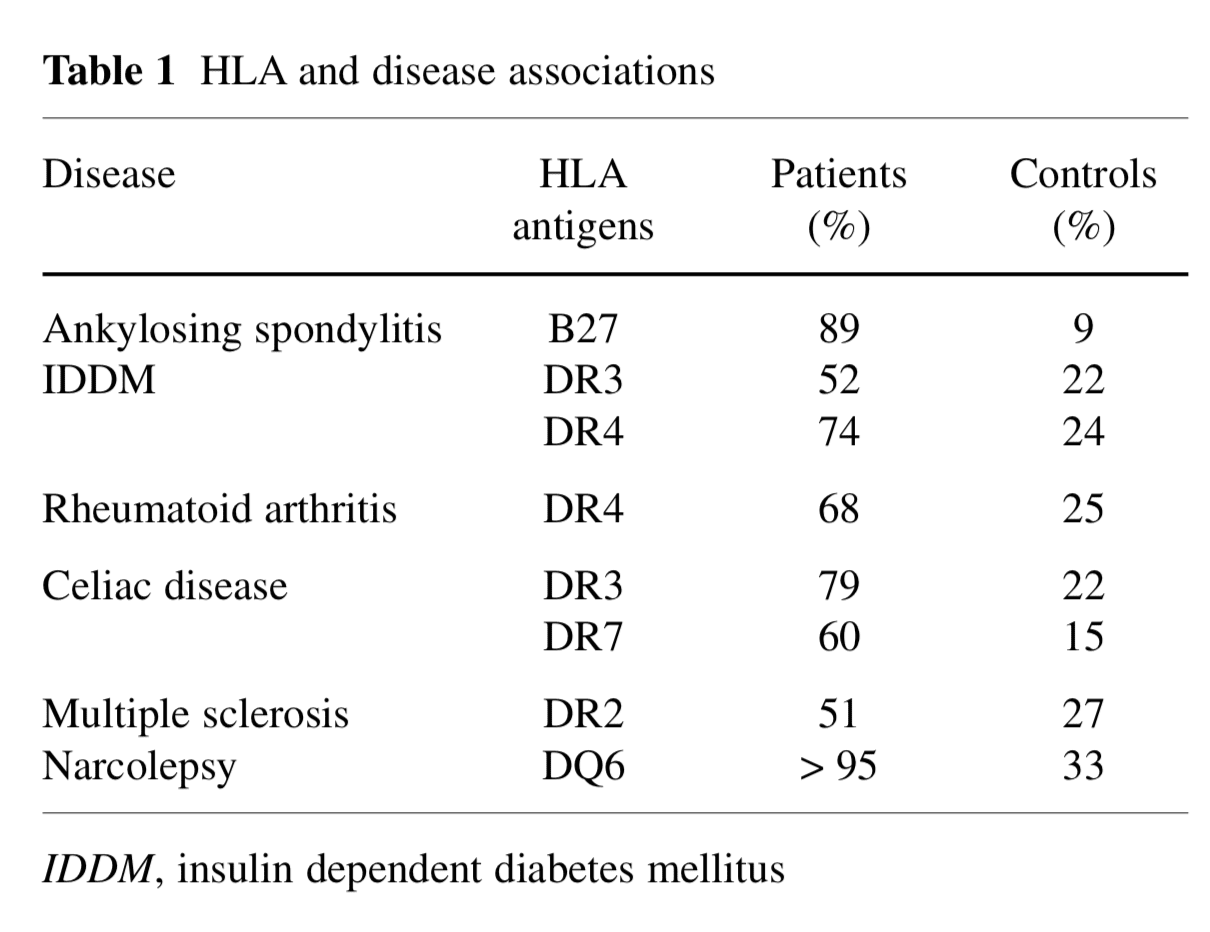
Narcolepsy — >95% of patients with narcolepsy-cataplexy carry HLA-DQB1*0602 (DQ6)

HLA stands for Human Leukocyte Antigen and refers to group of genes on chromosome 6 primarily involved in immune function (known as the Major Histocompatibility Complex – MHC)
Narcolepsy is a disorder categorised by excessive daytime sleepiness, despite adequate night-time sleep. It may be associated with cataplexy — a sudden loss of muscular tone that may lead to paroxysmal collapse, often brought on by excitement…. As this poodle demonstrates:
Other diseases linked to HLA are shown in the table below:
References
- Stanford Medicine – Narcolepsy Research FAQs
- Trabace S. HLA and disease association. J Headache Pain 2000;1:S109-S113
Question 4
Which snake has the most lethal venom in the world?
Reveal the funtabulous answer
The Inland Taipan (Oxyuranus microlepidotus), also known as the fierce snake or small-scaled snake.
The maximum venom yield recorded (for one bite) is apparently 110 mg. That would probably be enough to kill over 100 people or 250,000 mice (the mice would need to be standing very close together…)
Clinical manifestations of envenoming are (apart from potential death) venom-induced consumptive coagulopathy, neurotoxicity, as well as thrombocytopenia, microangiopathic hemolytic anemia and renal failure.
This shy elapid is rarely encountered — most human victims are herpetologists or reptile handlers. Chris Nickson had one case of an Inland Taipan envenoming — a man bitten by his pet snake… He had immaculate pressure immobilisation bandaging and turned up at the ED within 20 minutes of the bite. A fair few years later and we’re still waiting for his first blood sample to clot…

Reference:
- World Atlas – The most venomous snakes in the world
Question 5
What is the McGinn and White ECG sign?
Reveal the funtabulous answer
SI QIII TIII pattern – deep S wave in lead I, Q wave in III, inverted T wave in III. This “classic” finding is neither sensitive nor specific for pulmonary embolism; found in only 20% of patients with PE.
Drs Sylvester McGinn and Paul Dudley White (yes, of WPW fame…) published a series of nine patients in 1935, seven of which had the S1Q3T3 pattern:
Electrocardiograms taken soon after the occurrence of the pulmonary embolism showed similar changes in five of these patients, and, in two others taken some time after the attack….he changes that appear significant are the presence of a Q wave and late inversion of the T wave in Lead III… a prominent S wave… in lead I…In none of these cases was left axis deviation present at the time of the acute episode….
It is probable that the changes observe clinically and the electrocardiographic variations are due in large part to dilatation and partial failure of the chambers of the right side of the heart.
McGinn and White 1935
Other Key ECG findings for PE include:
- Sinus tachycardia – the most common abnormality; seen in 44% of patients.
- Complete or incomplete RBBB – associated with increased mortality; seen in 18% of patients.
- Right ventricular strain pattern – T wave inversions in the right precordial leads (V1-4) ± the inferior leads (II, III, aVF). This pattern is seen in up to 34% of patients and is associated with high pulmonary artery pressures.
- Right axis deviation – seen in 16% of patients. Extreme right axis deviation may occur, with axis between zero and -90 degrees, giving the appearance of left axis deviation (“pseudo left axis”).
- Dominant R wave in V1 – a manifestation of acute right ventricular dilatation.
- Right atrial enlargement (P pulmonale) – peaked P wave in lead II > 2.5 mm in height. Seen in 9% of patients.
- Clockwise rotation – shift of the R/S transition point towards V6 with a persistent S wave in V6 (“pulmonary disease pattern”), implying rotation of the heart due to right ventricular dilatation.
- Atrial tachyarrhythmias – AF, flutter, atrial tachycardia. Seen in 8% of patients.
- Non-specific ST segment and T wave changes, including ST elevation and depression. Reported in up to 50% of patients with PE.
Simultaneous T wave inversions in the inferior (II, III, aVF) and right precordial leads (V1-4) is the most specific finding in favour of PE, with reported specificities of up to 99% in one study.
Reference:
- McGinn S and White PD. Acute Cor Pulmonale Resulting From Pulmonary Embolism. JAMA 1935;104(17):1473-1480
…and finally


FFFF
Funtabulously Frivolous Friday Five
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.