
![]()
AV Block: 2nd degree, Mobitz II (Hay block)
Definition of Mobitz II block (Hay Block)
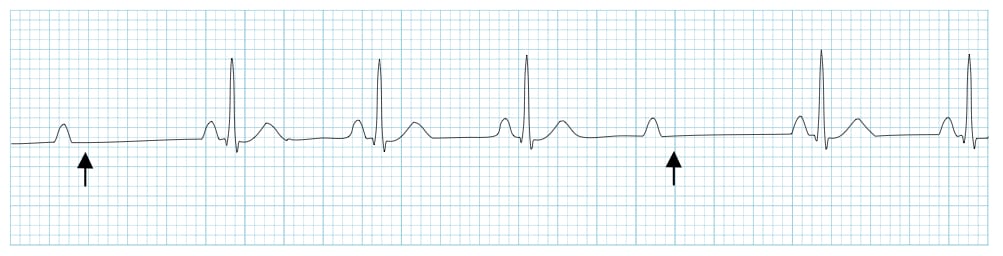
A form of 2nd degree AV block in which there is intermittent non-conducted P waves without progressive prolongation of the PR interval
Other features:
- The PR interval in the conducted beats remains constant
- The P waves ‘march through’ at a constant rate
- The RR interval surrounding the dropped beat(s) is an exact multiple of the preceding RR interval (e.g. double the preceding RR interval for a single dropped beat, triple for two dropped beats, etc)

Mechanism
- Mobitz II is usually due to failure of conduction at the level of the His-Purkinje system (i.e. below the AV node)
- While Mobitz I is usually due to a functional suppression of AV conduction (e.g. due to drugs, reversible ischaemia), Mobitz II is more likely to be due to structural damage to the conducting system (e.g. infarction, fibrosis, necrosis)
- Patients typically have a pre-existing LBBB or bifascicular block, and the 2nd degree AV block is produced by intermittent failure of the remaining fascicle (“bilateral bundle-branch block”)
- In around 75% of cases, the conduction block is located distal to the Bundle of His, producing broad QRS complexes.
- In the remaining 25% of cases, the conduction block is located within the His Bundle itself, producing narrow QRS complexes.
- Unlike Mobitz I, which is produced by progressive fatigue of the AV nodal cells, Mobitz II is an “all or nothing” phenomenon whereby the His-Purkinje cells suddenly and unexpectedly fail to conduct a supraventricular impulse.
- There may be no pattern to the conduction blockade, or alternatively there may be a fixed relationship between the P waves and QRS complexes, e.g. 2:1 block, 3:1 block.
Causes of Mobitz II
- Anterior MI (due to septal infarction with necrosis of the bundle branches)
- Idiopathic fibrosis of the conducting system (Lenègre-Lev disease)
- Cardiac surgery, especially surgery occurring close to the septum e.g. mitral valve repair
- Inflammatory conditions (rheumatic fever, myocarditis, Lyme disease)
- Autoimmune (SLE, systemic sclerosis)
- Infiltrative myocardial disease (amyloidosis, haemochromatosis, sarcoidosis)
- Hyperkalaemia
- Drugs: beta-blockers, calcium channel blockers, digoxin, amiodarone
Clinical Significance
- Mobitz II is much more likely than Mobitz I to be associated with haemodynamic compromise, severe bradycardia and progression to 3rd degree heart block
- Onset of haemodynamic instability may be sudden and unexpected, causing syncope (Stokes-Adams attacks) or sudden cardiac death
- The risk of asystole is around 35% per year
- Mobitz II mandates immediate admission for cardiac monitoring, backup temporary pacing and ultimately insertion of a permanent pacemaker
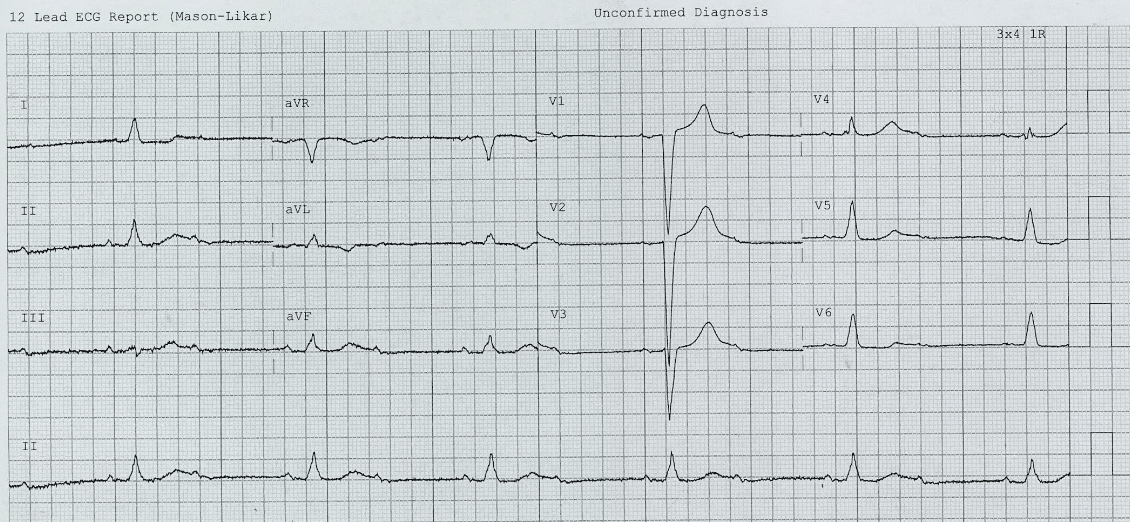
Examples
ECG 1
Related Topics
- AV block: 1st degree
- AV block: 2nd degree, Mobitz I
- AV block: 2nd degree, “fixed ratio blocks” (2:1, 3:1)
- AV block: 2nd degree, “high grade AV block”
- AV block: 3rd degree (complete heart block)
- Eponymythology: History of Second-degree AV block. 2020
- Eponym: Karel Frederik Wenckebach (1864 -1940). LITFL 2020
- Eponym: Woldemar Mobitz (1889 – 1951). LITFL 2020
- Eponym: John Hay (1873 – 1959). LITFL 2020
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner
Thank you very much for your site! I’am a 25years-experience-old nurse and I have been an EMT for 11years in Montreal, Canada. I looooooove the quality and clarity of your descriptions of any cardiac rhythms I read about.
I’am currently working as a nursing educator. I recommand your site to ALL the young/old any nurses/lpn I worked with.