
![]()
ECG Case 130
Thanks to Emergency Physician Dr David McCreary for sharing this case for discussion.
Another busy night in ED and another ECG is thrust in front of you.
25-year-old female with ‘palpitations’. BP 117/72, GCS 15.
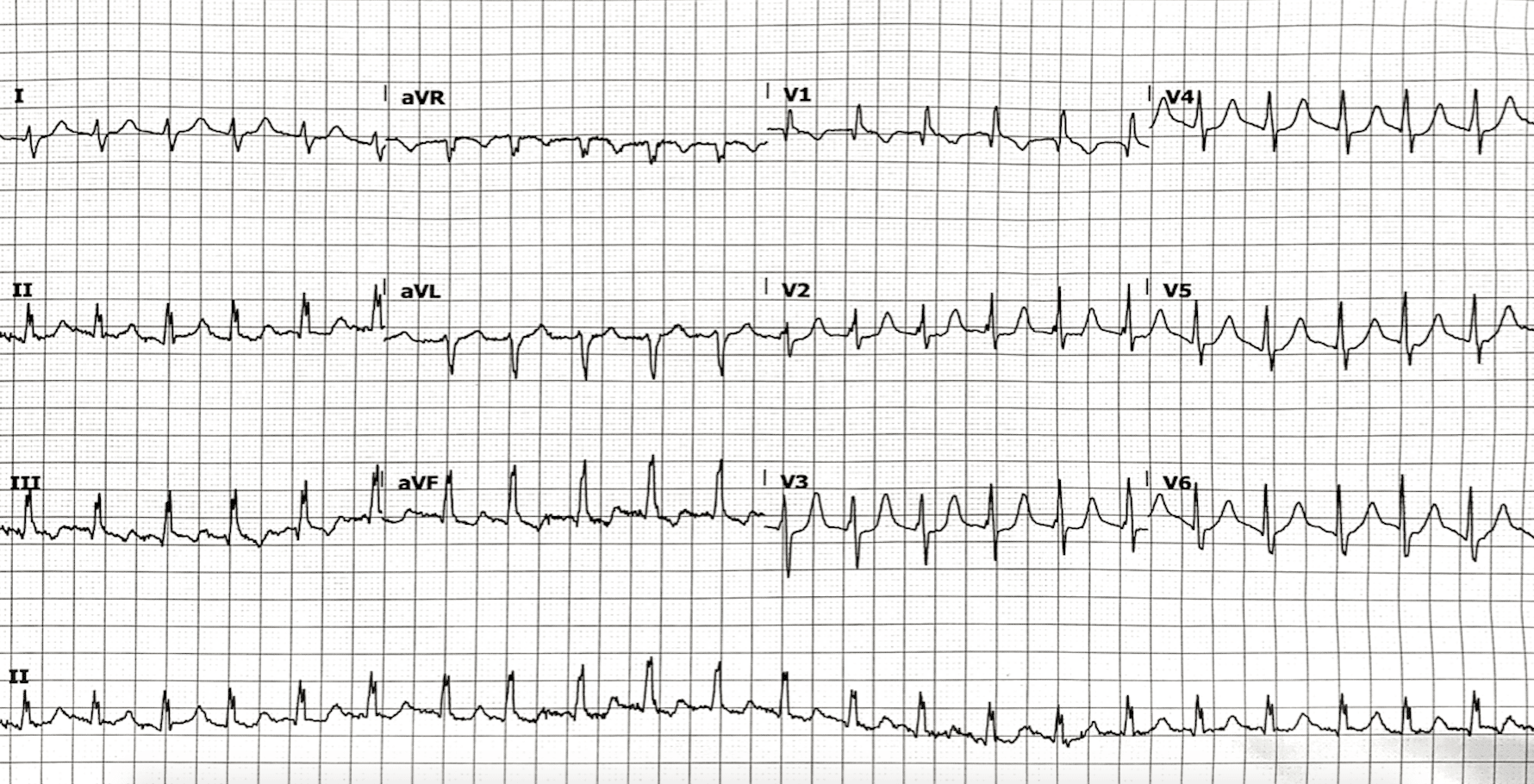
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
- Regular narrow complex tachycardia, rate 132 bpm
- Slight right axis deviation
- Dominant R wave in V1 meets voltage criteria for right ventricular hypertrophy (RVH)
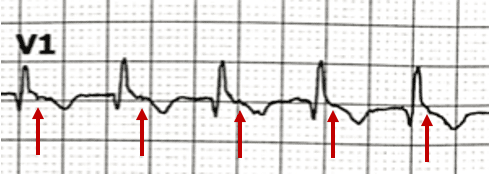
- Pseudo R’ waves in the terminal portion of the QRS in V1, an isoelectric baseline, and lack of flutter waves in V1 point towards this rhythm being an AV nodal re-entry tachycardia (AVNRT)
- No rate-related ischaemia
There is one other feature on this ECG that suggests this patient has a congenital structural abnormality, can you spot it?
Reveal answer
- Notching near the apex of the R wave in inferior leads is known as Crochetage sign
- The presence of this sign in all three inferior leads has a 92-100% specificity for the diagnosis of a secundum atrial septal defect (ASD)

Shortly after the above ECG was taken, the patient spontaneously reverted into sinus rhythm and a repeat ECG was taken:

What is your interpretation?
Reveal answer
- Normal sinus rhythm, rate 84 bpm
- Multiple premature atrial complexes (PACs) — 2nd and 10th beat
- Features of secundum ASD are again seen — Crochetage sign in all three inferior leads, slight RAD and dominant R wave in V1
OUTCOME
This patient self-reverted in and out of AVNRT multiple times during her stay in the emergency department. When in sinus rhythm she had frequent PACs, which reduced following the administration of metoprolol. She subsequently remained in sinus rhythm and was referred for formal TTE and evaluation for definitive repair of secundum ASD.
CLINICAL PEARLS
Secundum ASD is a common sporadic congenital heart defect with a prevalence of around 1 in 800 in the general population. Patients with an isolated defect usually remain asymptomatic until the 3rd decade of life, with the most common adult presentation being supraventricular tachycardia (SVT), followed by exercise intolerance and/or fatigue. If left untreated, long term morbidity relates to the development of pulmonary hypertension.
ECG changes likely relate to functional RV volume overload due to left-to-right shunting, with resultant raised pulmonary pressures. The characteristic Crochetage sign often disappears following defect repair, which is usually via transcatheter device closure.
ECG features of secundum ASD
- Characteristic R wave notching in inferior leads (Crochetage sign)
- Slight right axis deviation (RAD)
- Voltage evidence of right ventricular hypertrophy (RVH), often in the form of “incomplete” right bundle branch block (RBBB)
Differentials for “SVT” in this patient
The term “SVT” is a misnomer commonly used synonymously with AVNRT, which is one of many forms of SVT. SVT refers to any tachyarrhythmia arising from above the level of the Bundle of His, and encompasses regular atrial, irregular atrial, and regular atrioventricular tachycardias.
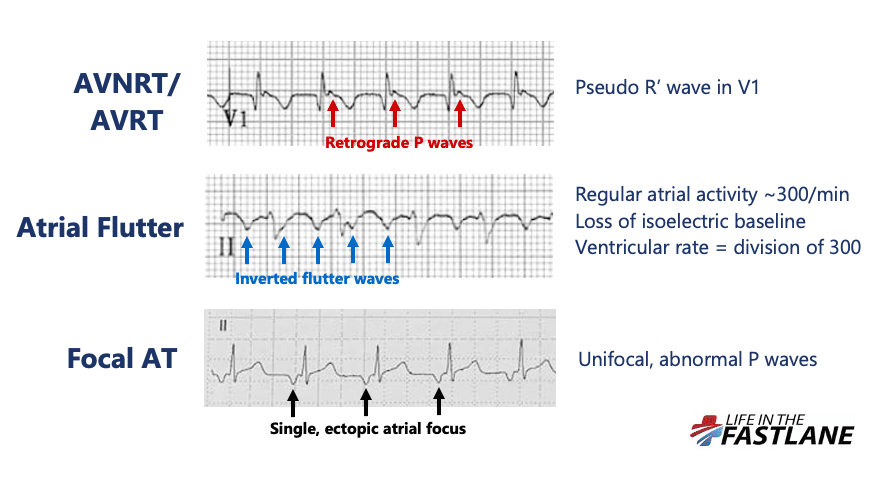
Differentials for a regular narrow complex tachycardia include:
The most common form of AVNRT (slow-fast) is precipitated by the arrival of a PAC whilst the AV node is still refractory. This leads to the formation of a re-entry circuit, which causes simultaneous anterograde activation of the Bundle of His and retrograde activation of the atria. Resultant HR will depend on the length of the re-entry circuit in the AV node which is variable between patients.
The presence of retrograde P waves on the ECG is variable – they may be buried within or after the QRS complex. The term pseudo R’ wave refers to the presence of a retrograde P wave visible in the terminal portion of the QRS complex, usually best seen in V1 or V2, which may mimic an RSR’ complex appearance. These can be very subtle.
Differentiation of AVNRT from atrial flutter on the ECG can be difficult and may not always be possible. Atrial flutter is caused by a similar re-entry circuit occurring within the right atrium. The length of this circuit corresponds to the size of the right atrium, usually resulting in flutter waves at a rate of ~300bpm. The ventricular rate depends on the AV conduction ratio. This ratio is often referred to as the “AV block”, however this is again a misnomer. Such AV bock is a physiological response to rapid atrial rates and implies a normally functioning AV node.
High grade AV conduction ratios in atrial flutter (4:1, 5:1), particularly with variable block, are often seen in the presence of AV nodal blocking drugs in the elderly population.
- When present in all three inferior leads, Crochetage sign is highly specific for the diagnosis of secundum ASD
- Commonly used to refer to AVNRT, SVT is a broad term encompassing regular atrial, irregular atrial, and regular atrioventricular tachycardias
- At rates of ~150bpm, differentiation of AVNRT versus atrial flutter can be difficult. Look for pseudo R’ waves in V1 suggestive of AVNRT, or consider the use of adenosine which will revert AVNRT or unmask flutter waves in atrial flutter
Further reading
Related topics
References
- van der Linde et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol. 2011 Nov 15;58(21):2241-7
- Engelfriet et al. Repaired and open atrial septal defects type II in adulthood: an epidemiological study of a large European cohort. Int J Cardiol. 2008 Jun 6;126(3):379-85
TOP 150 ECG Series

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.

Interventional cardiologist, ECG and hemodynamics fan. MD, Assoc. Prof. at Marmara University, Pendik T&R Hospital, Assoc. Editor at Archives of TSC, ESC National Prevention Coordinator
Very interesting Case, first i thought of WPW because of V2/V3 seem to have Delta Waves so AVRT. But very happy to learn about the Crochetage sign.
Can AVNRT have some irregularities in the RR interval?… As this one clearly does. Especially at avF. Please explain.. Thanks