
![]()
Non-traumatic Abdominal Ecchymosis
Eponymythology: The myths behind the history
We review the original descriptions of 5 eponymous signs associated with non-traumatic bruising related to intra-abdominal pathology.
These commonly cited eponyms involving the abdominal wall and flanks (Grey Turner, Cullen and Stabler); scrotum (Bryant) and upper thigh (Fox) may be useful clues directing the examiner to consider potentially serious causes of abdominal pathology.
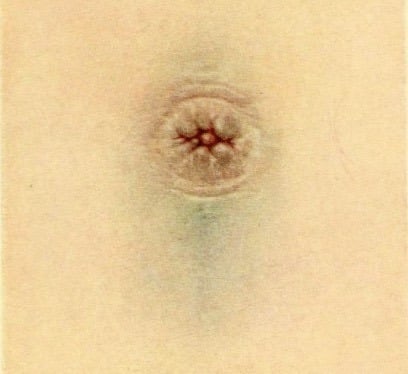
Cullen sign
Non-traumatic peri-umbilical ecchymoses associated with intra-abdominal haemorrhage, originally described in ectopic pregnancy
1918 – Thomas Stephen Cullen (1869-1953) first described a bluish black discolouration of the periumbilical skin in a female patient with a ruptured extrauterine pregnancy with ‘no history of injury‘
He concluded that the umbilical appearance was due to intra-abdominal haemorrhage secondary to an ectopic pregnancy. He originally described the finding at the 43rd annual meeting of the Transactions of the American gynecological society, Pennsylvania May 16-18, 1918
The patient, a woman, thirty-eight years of age, suddenly developed abdominal pain and distention. Dr. Cullen saw her three weeks later. The umbilical region was bluish black, although she gave no history of injury. Vaginal examination yielded nothing on account of the abdominal distention. Under ether, however, a mass 8 X 6 cm. was clearly felt to the right of the uterus. Dr. Cullen at once diagnosed extrauterine pregnancy, although the patient had missed no period and there was no uterine bleeding. On opening the abdomen he found a right-sided extrauterine pregnancy and about one and a half quarts of free blood in the abdomen.
Cullen TS 1918
Cullen expanded on this report in Contributions to Medical and Biological Research, a two volume tome dedicated to Sir William Osler on the occasion of his seventieth birthday on July 12, 1919.
Bearing Dr. Ransohoff’s 1905 case in mind I dictated the following note prior to opening the abdomen: “The bluish black appearance of the navel unassociated with any history of injury, together with the mass to the right of the uterus, makes the diagnosis of extrauterine pregnancy relatively certain.”
Cullen TS 1919
Cullen 1919: 420-422
Clinical context
- Despite the original description, most literature relates Cullen sign of periumbilical ecchymosis to acute pancreatitis (being recorded in 1-3% cases) rather than secondary to an ectopic pregnancy.
- In most described cases, it takes 3-5 days for Cullen sign to present and the sign been associated with a broad range of clinical conditions
Alternate causes for Cullen Sign
| Cause | Reference |
|---|---|
| Retroperitoneal necrotizing fasciitis | Pryor et al 2001 |
| Strangulated umbilical hernia | Orient JM, Sapira JD 2005 |
| Strangulation of ileum with hemorrhage | Orient JM, Sapira JD 2005 |
| Renal sarcoma metastatic to the peritoneum | Orient JM, Sapira JD 2005 |
| Ovarian cyst hemorrhage | Orient JM, Sapira JD 2005 |
| Hypothyroid myopathy | Orient JM, Sapira JD 2005 |
| Hepatocellular carcinoma | Orient JM, Sapira JD 2005 |
| Cirrhosis with portal hypertension | Orient JM, Sapira JD 2005 |
| Bilateral acute salpingitis with IUP | Orient JM, Sapira JD 2005 |
| Hemorrhaging ascites from hepatic tumor | Mabin, Gelfand 1974 |
| Ischemic and gangrenous bowel | Kelley ML 1961 |
| Rectus sheath hematoma | Guthrie, Stanley 1996 |
| Perforated duodenal ulcer | Evans DM 1971 |
| Splenic rupture | Chung et al 1992 |
| Percutaneous liver biopsy | Capron et al 1977 |
| Acute Pancreatitis | Bosmann et al 2009 |
| Ruptured abdominal aortic aneurysm | Armour et al 1978 |
- Epperla N, Mazza JJ, Yale SH. A Review of Clinical Signs Related to Ecchymosis. WMJ. 2015; 114(2): 61-65.
Grey Turner sign
Non-traumatic abdominal ecchymosis, in particular – bruising of the flanks associated with retroperitoneal haemorrhage, originally described in acute pancreatitis
1920 – The English surgeon George Grey Turner (1877–1951) published paper on ‘Local discoloration of the abdominal wall as a sign of acute pancreatitis‘ citing two cases of acute pancreatitis with fat necrosis and retroperitoneal haemorrhage.
Case 1 [1912]
54 year old female with three days of abdominal pain presenting with an area of discoloration (a bluish colour), about 6 inches in diameter involving the abdominal wall surrounding the umbilicus (see Cullen sign…)
…the patient suffered from acute pancreatitis, with much effusion into the peritoneal cavity. She lived nine days after operation, and the post-mortem examination disclosed a sloughing pancreas with much fat necrosis
Grey Turner 1920
Case 2 [1917]
53 year old male soldier with a history of recurrent bouts of self-limiting abdominal pain. He presented with unremitting abdominal pain and a rigid abdomen…looking ‘distinctly toxic’
The tenderness over the gall-bladder region was very marked, and I now noticed two large discoloured areas in the loins. They were about the size of the palm of the hand, slightly raised above the surface, and of a dirty-greenish colour.
Grey Turner 1920

Clinical context
- Incidence of 3-5% in patients with acute pancreatitis, associated with increased mortality (30-40%) and increased risk of pseudocyst formation. [Surg Gynecol Obstet. 1984]
- CT scanning has helped to define the anatomic pathway by which extravasated pancreatic enzymes and their effects lead to these cutaneous discolorations. [Pancreas. 1998.]. Extraperitoneal diffusion from the anterior pararenal space between the two leaves of the posterior renal fascia; to the lateral edge of the quadratus lumborum muscle and may then extend to the posterior pararenal space and the structures of the flank wall. The lumbar triangle, a site of anatomic weakness on the flank wall, provides an external window into the internal proteolytic events.
- In most described cases, it takes 3-5 days for Grey Turner sign to present and the sign been associated with a broad range of clinical conditions
Alternate causes for Grey Turner Sign
| Cause | Reference |
|---|---|
| Intra-aortic balloon pump insertion | Rob, Williams 1961 |
| Cardiac catheterization | Armour et al 1978 |
| Sclerosing peritonitis | Pryor et al 2001 |
| Rectus sheath hematoma | Guthrie, Stanley 1996 |
| Ruptured abdominal aortic aneurysm | Armour et al 1978 |
| Retroperitoneal necrotizing fasciitis | Pryor et al 2001 |
| Ischemic and gangrenous bowel | Kelley ML 1961 |
| Bilateral acute salpingitis with IUP | Orient JM, Sapira JD 2005 |
| Acute Pancreatitis | Bosmann et al 2009 |
- Epperla N, Mazza JJ, Yale SH. A Review of Clinical Signs Related to Ecchymosis. WMJ. 2015; 114(2): 61-65.
Stabler sign
Non-traumatic abdominal skin ecchymosis in the inguinal-pubic area associated with intra-abdominal haemorrhage, originally described in ectopic pregnancy
1934 – Francis Edward Stabler (1902-1967) published a paper titled ‘A case showing Cullen’s sign‘ concerning a patient presenting with an ectopic pregnancy: with left illiac fossa pain of fourteen days duration and ilioinguinal ‘bruising’, 7 weeks post last menstrual period.
Clinical examination
C.S. Aged 34: One inch below and to the left of the umbilicus was a purple, almost black, clearly cut mark 3/4 in. by 1/4 in. shaped like a comma. Below it, about the junction of the upper third and lower two-thirds of the distance from the umbilicus to the pubes, was a ” bruise,” bluish in colour, about 1 in. in diameter, whilst abutting on the inguinal fold was a reddish-purple mark like a fresh bruise, shaped roughly like the ace of clubs, about 2 in. in diameter. The whole was within the triangle formed by the midline and a line drawn to the umbilicus from the middle of the left inguinal ligament. On bimanual examination a soft mass the size of a hen’s egg was evident in the left tubal region.
Operative findings
At operation the distal half of the left Fallopian tube contained an ampullary pregnancy surrounded by blood clot. The tube was not ruptured, but a little dark blood was oozing from the abdominal ostium. In the peritoneal cavity there were not more than 3 or 4oz (88-118mL) of dark fluid blood…incision into the subcutaneous fatty tissue proved the stains to be true ecchymoses.
Hypotheses
It is an interesting speculation as to how the blood reaches the subcutaneous tissues. In the present reported case I forecast that there would be an intraligamentary rupture of the tube with a broad ligament haematoma from which blood had tracked up extraperitoneally as far as the umbilicus, possibly following the obliterated hypogastric artery by which the lateral spread of the discoloration was limited.
Clinical context
Initially described as an inguinal-pubic extension of the peri-umbilical ecchymosis of Cullen sign. Further cases of bruising to the inguinal-pubic area reported with AAA rupture and acute hemorrhagic pancreatitis
Although rare, this sign has most commonly been identified in neonates secondary to adrenal hemorrhage. This is associated with obstetric injury, perinatal hypoxia, and sepsis [Urology. 2002]. Rarely, it may be due to ruptured neuroblastoma.
Fox’s sign
Non-traumatic ecchymosis over the upper outer aspect of the thigh. Ecchymosis is parallel with, but distal to the inguinal ligament with a well demarcated upper border defined by attachment of the membranous layer of the superficial fascia (Scarpa’s fascia).
1966 – John Adrian Fox (1933-2018) detailed 2 fatal cases of non-traumatic ecchymosis determined as a diagnostic sign of retroperitoneal haemorrhage. In both cases, this sign was noticed late in the course and produced by tracking of the fluid extraperitoneally along the fascia of psoas and iliacus beneath the inguinal ligament until it became subcutaneous in the upper thigh.
Case 1: [Post mortem: acute suppurative pancreatitis]
Fourteen hours after admission bruising was noted in both upper outer thighs. It had a sharp upper margin, was dark blue, and was quite distinct from the patchy mottling of her legs below.

Case 2: [Post-mortem: dissecting and ruptured abdominal aortic aneurysm]
A man, of about 50…with severe abdominal pain and circulatory collapse. Resuscitatory measures were of no avail and he died within 24 hours of admission. Before death bruising was noticed in the upper outer aspect of one thigh. He had not been given injections in this region and no other cause for the bruising was apparent.
Hypotheses and cadaver experiment
.. it seems likely that the clinical sign seen in the above 2 cases is produced by tracking of the fluid extraperitoneally along the fascia of psoas and iliacus beneath the inguinal ligament until it becomes subcutaneous in the upper thigh.
This sign has been reproduced in two stages in the recent cadaver. A solution of methylene blue in normal saline was injected from a height of 10 feet into the loin for several hours. The blue dye was then traced by dissection until it was seen to pass beneath the inguinal ligament”
Clinical context
Initially recorded in acute pancreatitis and ruptured aortic aneurysm. Subsequently described with strangulated ileum, urethral instrumentation, reaction to subcutaneous injections, and pulmonary infarction.
Resources
- John Adrian Fox (1933-2018) was an English surgeon
- Fox JA. A diagnostic sign of extraperitoneal hemorrhage. Br J Surg. 1966; 53(3): 193-195
Bryant sign
Scrotal ecchymosis associated with ruptured abdominal aortic aneurysm (AAA)
1903 – John Henry Bryant (1867–1906) described scrotal ecchymosis associated with ruptured AAA during two lectures in which he had evaluated 18,678 necropsies and the 325 deaths secondary to abdominal aortic aneurysm rupture.
{kind=link}
In these two articles Bryant describes the diffuse nature of the atheromatous changes, the possible clinical presentation of AAA as apparent renal colic, and the scrotal and abdominal discolourations as diagnostic clues
In one case blood was effused into the right spermatic cord, and the corresponding half of the scrotum was much ecchymosed…When blood is extravasated into the anterior abdominal wall ecchymoses may appear…
Bryant, Clin Jour. 1903
JH Bryant original description
Most recorded cases of Bryant sign occur three to six days after onset of abdominal symptoms – Pearlman (1940), Barratt-Boyes (1957) and Beebe (1958).
1987 – RM Ratzan et al proposed eponymous historical attribution of lower abdominal/scrotal discolouration secondary to aortic aneurysmal disease to John Henry Bryant. [J Emerg Med. 1987 Jul-Aug;5(4):323-9]
Clinical context
Bryant sign is rare. Blood must transverse the inguinal canal and spermatic cord down to the subcutaneous scrotal tissue.
It requires specific pathological circumstances such as a closed (retroperitoneal hematoma) or sealed (surrounding retroperitoneal and aortic tissue) rupture of abdominal aortic aneurysm. It requires a slow rate of aneurysmal leakage and a prolonged interval prior to final rupture.
Bryant Blue Scrotum sign [**graphic content warning]

Summary
The original publications of the eponymised cases often include careful clinical descriptions and anatomopathophysiological hypotheses in an era devoid of adjunctive diagnostic aids. However, we now have the benefit of comparing the diagnostic validity of the signs in a vast array of published clinical cases illuminated by enhanced imaging techniques and a more in-depth understanding of pathophysiology.
The original n=1 published cases represent a springboard for us to review arcane terminology by first understanding the historical folksonomy and then to redefine in clinical context to reduce descriptive confusion and narrowing of our diagnostic differentials.
For example, in 1918 Cullen described a single case of umbilical ecchymoses in a patient with an ectopic pregnancy. Over the subsequent 100 years at least 17 alternate diagnoses have been ascribed to the external abdominal manifestation of his eponymous sign.
Of significant note, the topographic location of atraumatic abdominal ecchymosis does not point to the aetiology with any degree of certainty and these signs may be potentiated by anticoagulation therapy or qualitative/quantitative platelet abnormalities.
Of course there is a certain historical interest in relating these signs to pioneers in descriptive medicine. However, we may be better to describe ‘non-traumatic abdominal wall ecchymosis’ as a potential sign of intraperitoneal or retroperitoneal pathology which requires further evaluation…
References
Original articles
- Cullen TS. A new sign in ruptured extrauterine pregnancy. American journal of obstetrics and diseases of women and children. 1918; 78: 457
- Cullen TS. Bluish discolouration of the umbilicus as a diagnostic sign when ruptured extrauterine pregnancy exists. In: Contributions to Medical and Biological Research. 1919; 1: 420-422
- Grey Turner G. Local discoloration of the abdominal wall as a sign of acute pancreatitis. Br J Surg. 1920;7:394-395
- Stabler F. A case showing Cullen’s sign. Br Med J. 1934;2(3840):255-256.
- Fox JA. A diagnostic sign of extraperitoneal haemorrhage. Br J Surg. 1966 Mar;53(3):193-5.
- Bryant JH. Two clinical lectures on aneurysm of the abdominal aorta: lecture 1. The Clinical Journal. 1903; 23: 71-80.
- Epperla N, Mazza JJ, Yale SH. A Review of Clinical Signs Related to Ecchymosis. WMJ. 2015; 114(2): 61-5.
FOAMed resources
- Cadogan M. Cullen sign: Eponym A Day. Instagram
- Cadogan M. Fox’s sign: Eponym A Day. Instagram
- Cadogan M. Grey Turner sign: Eponym A Day. Instagram
eponymythology
the myths behind the names
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |