
![]()
ECG Case 054
Elderly patient presenting with nausea and visual disturbance. Interpret the ECG.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
This is a tricky ECG!
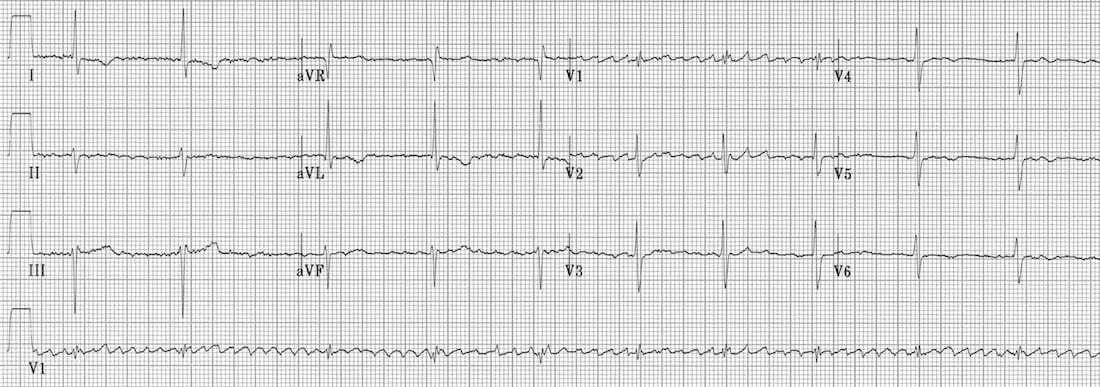
There is evidence of atrial fibrillation, as evidenced by the irregular baseline with fibrillatory waves most prominent in V1-2.
NB. Fibrillatory waves are characteristically seen in V1-2 (which overlie the atria), as opposed to tremor artefact which may be in seen in multiple leads without a predominance for V1-2.
However, the ventricular rhythm is regular. How can this be? AF is irregular by definition…
This is an example of “regularised AF” due to digoxin toxicity:
- The underlying rhythm is AF, which is being treated with digoxin.
- There is complete heart block, prevent atrial impulses from reaching the ventricles.
- There is an accelerated junctional rhythm maintaining cardiac output.
If this all seems like too much of a coincidence, then consider the pathophysiology of digoxin toxicity…
CLINICAL PEARLS
Mechanisms of Digoxin Toxicity
Digoxin toxicity produces a wide variety of dysrhythmias, due to:
- Increased automaticity of atrial, junctional and
ventricular tissues — via actions at the Na/K and Na/Ca exchangers
causing increased intracellular calcium and therefore increased
spontaneous depolarisation of cardiac pacemaker cells. - Decreased AV conduction — via increased vagal tone at the AV node.
Digoxin toxicity produces some combination of:
- Increased atrial automaticity — especially atrial tachycardia, but also atrial ectopics, AF, flutter.
- Increased junctional automaticity — especially accelerated junctional rhythms.
- Increased ventricular automaticity — frequent VEBs and bigeminy, polymorphic VT.
- AV blocks — including 1st, 2nd and 3rd degree AV block.
Characteristic ECG patterns include:
- Atrial tachycardia with high-grade AV block (= the classic dig-toxic rhythm).
- Regularised AF = AF with complete heart block + accelerated junctional escape rhythm, producing a paradoxically regular rhythm.
- Bidirectional VT = polymorphic VT with QRS complexes that alternate between left- and right-axis-deviation, or between LBBB and RBBB morphology.
NB. Digoxin toxicity should not be confused with digoxin effect (= “sagging” ST depression and T-wave inversion in patients on therapeutic doses of digoxin; not predictive of toxicity).
Clinical Pearls
- Check for tremor artefact before you start diagnosing regularised AF!
- If the ECG pattern appears genuine and the clinical picture is
compatible with digoxin toxicity (GI upset, xanthopsia, current digoxin
treatment), then check an urgent digoxin level.
References
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 100 ECG Series
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |
Heyo,
I love your site.
Im a little confused by the diagnosis of that ecg.
Couldn‘t this be an atrial flutter ? (which in most of the cases is regular ).
The waves between the QRS Komplexes are so big and regular.
Greetings from germany
Daniel
Why cant it be atrial flutter??