
![]()
ECG Case 030
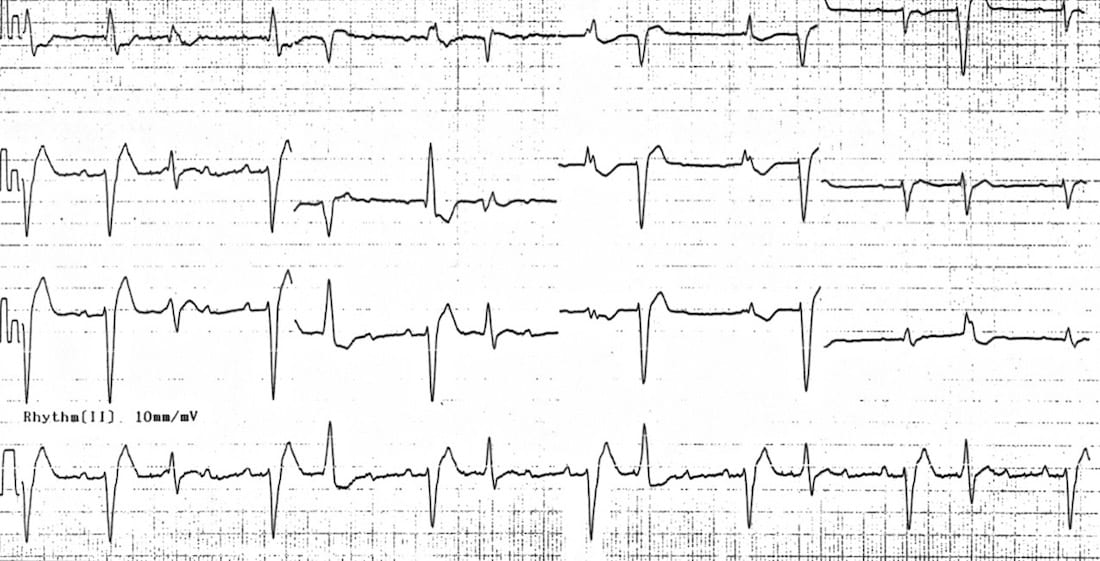
85-year old patient presenting with nausea, vomiting and visual disturbance. Looks clinically dehydrated. Describe the ECG.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Main Abnormalities
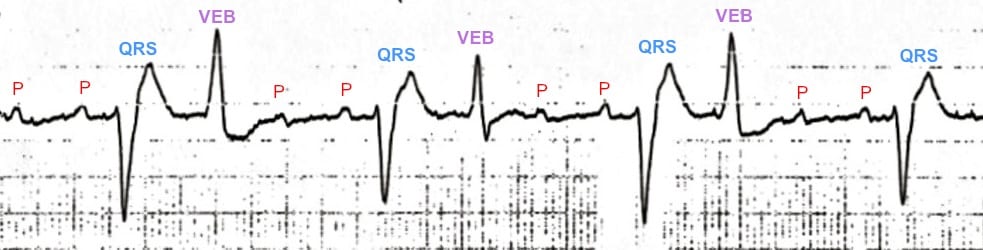
- Atrial tachycardia, with regular P waves visible at ~ 160 bpm (many of the P waves are hidden within T waves and VEBs)
- Evidence of high-grade AV block — there is a 4:1 conduction ratio between P waves and QRS complexes, with a QRS rate of ~ 40 bpm
- Frequent ventricular ectopic beats occurring in a pattern of ventricular bigeminy
- Alternating LBBB and RBBB morphology, with the conducted QRS complexes demonstrating RBBB morphology (RSR’ in V1) and the VEBs demonstrating LBBB morphology (dominant S wave in V1)
Diagnosis
The combination of…
- Atrial tachycardia
- Frequent ventricular ectopic beats
- High-grade AV block
… is almost pathognomonic of severe digoxin toxicity.
CLINICAL PEARLS
ECG Features of Digoxin Toxicity
Digoxin toxicity produces a wide variety of dysrhythmias, due to:
- Increased automaticity of atrial and ventricular tissues — via actions at the Na/K and Na/Ca exchangers causing increased intracellular calcium and therefore increased spontaneous depolarisation of cardiac pacemaker cells
- Decreased AV conduction — via increased vagal tone at the AV node
Digoxin toxicity therefore usually produces some combination of:
- Increased atrial automaticity — especially atrial tachycardia, but also atrial ectopics, AF, flutter
- Increased ventricular automaticity — frequent VEBs and bigeminy, polymorphic VT
- AV blocks — including 1st, 2nd and 3rd degree AV block
Characteristic ECG patterns include:
- Atrial tachycardia with high-grade AV block (= the classic dig-toxic rhythm)
- “Regularised AF” = AF with complete heart block + accelerated junctional escape rhythm, producing a paradoxically regular rhythm
- Bidirectional VT = polymorphic VT with QRS complexes that alternate between left- and right-axis-deviation, or between LBBB and RBBB morphology
NB. Digoxin toxicity should not be confused with digoxin effect (= “sagging” ST depression and T-wave inversion in patients on therapeutic doses of digoxin; not predictive of toxicity).
References
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 100 ECG Series
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.

Thank you for your enjoyable quiz. I’ve some other opinions on the interpretation.
1. I think there is no clues for atrial tachycardia except for the high atrial rate when the patient’s age comes in. The axis of P-wave looks normal.
2. There is a Mobitz-type of 2nd-degree AV block (3:2 conduction).
3. For each couplet, the first complex has a bifascicular appearance. There are underlying conduction abnormalities including RBBB and left anterior hemiblock.
4. For each couplet, the second complex has variable morphologies. This is due to the fusion from the above-mentioned complex and a ventricular extrasystole from the right ventricle.
In summary, this ECG presents 1) Mobitz-type of 2nd-degree AV block with 3:2 conduction, 2) Underlying RBBB + Left anterior hemiblock, 3) RV-origin ventricular extrasystoles in a bigeminy fashion.
Can the second complex in each couplet be alternating capture vs fusion beats ?