![]()

Philip Allison
Philip R. Allison (1907–1974), pioneering thoracic surgeon, defined reflux oesophagitis, advanced Barrett’s oesophagus, and led Oxford surgery

![]()
Philip R. Allison (1907–1974), pioneering thoracic surgeon, defined reflux oesophagitis, advanced Barrett’s oesophagus, and led Oxford surgery
Norman Barrett (1903–1979), thoracic surgeon, pioneer of oesophageal surgery, first repair of Boerhaave’s syndrome, and namesake of Barrett’s oesophagus.

Emergency Procedure: closing lacerations. Three updated videos covering the Simple Suture, Advanced Skills and Stapling
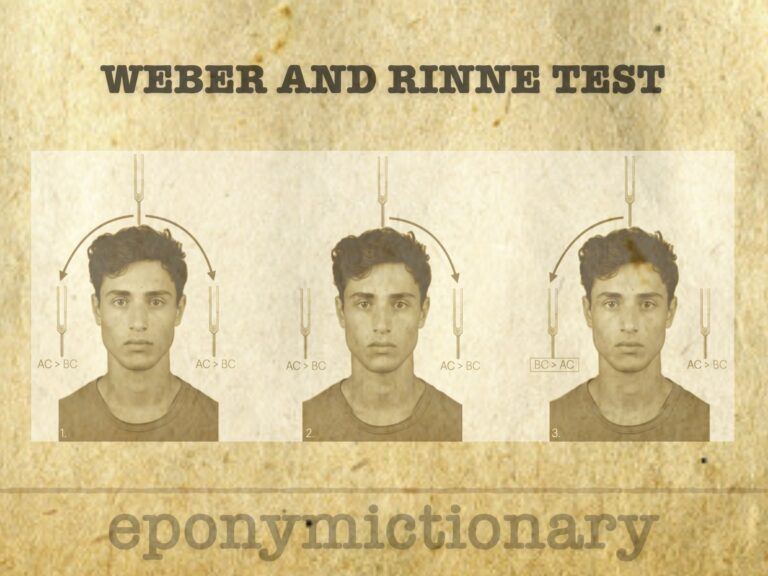
The Weber and Rinne tuning fork tests differentiate conductive from sensorineural hearing loss using the principles of bone and air conduction.
Pioneer of the Allen test and anticoagulant therapy, Edgar V. Allen (1900–1961) advanced vascular medicine with key insights into dicumarol use and lipedema
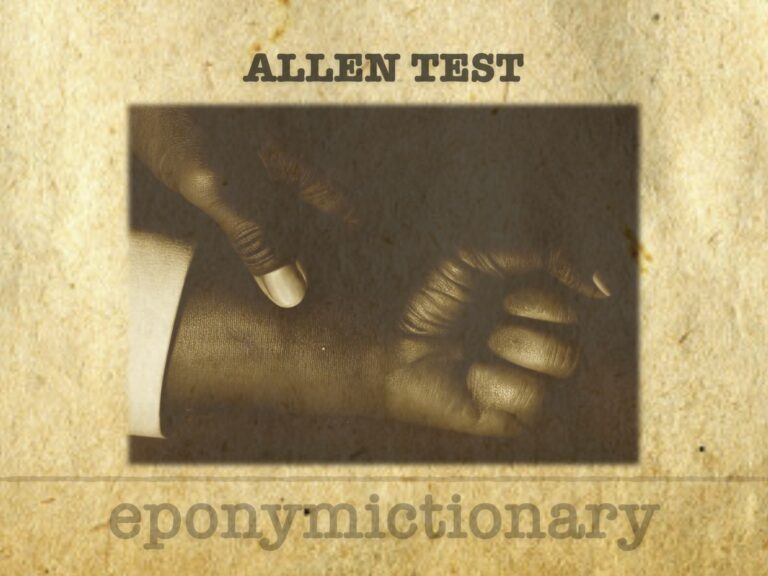
Allen Test: a bedside exam assessing hand arterial flow via radial/ulnar patency; used before ABG, cannulation, or radial artery harvest.
Sir James Mackenzie (1853–1925), Scottish GP and pioneer cardiologist, invented the ink polygraph and defined arrhythmias, angina, and atrial fibrillation
Yvonne Margaret (née Barr) Balding (1932 - 2016) was an Irish virologist. Co-discoverer of Epstein–Barr virus (EBV) (1964)
Henri Huchard (1844–1910), French cardiologist at Necker, defined “cardio-arterial” disease, described Huchard’s sign, and helped shape early hypertension care.
Alexander Tietze (1864–1927), German surgeon who described Tietze syndrome. Expert in emergency surgery and civic leader in Breslau during WWI.
W.N. Pickles (1885–1969), rural GP and epidemiologist, defined Bornholm disease in Britain and shaped modern public health through detailed field observation.

Texidor’s Twinge (Precordial Catch Syndrome): benign, sharp chest pain in youth, first described in 1892, clarified by Miller, Texidor, and Asher in the 1950s.