
![]()
De Winter T Wave
First reported by Dutch Professor of Cardiology, Robbert J. de Winter in 2008, the de Winter ECG pattern is an anterior STEMI equivalent that presents without obvious ST segment elevation. These patients are suffering occlusion myocardial infarction (OMI) and require immediate reperfusion therapy.
ECG Diagnostic Criteria
- Tall, prominent, symmetrical T waves in the precordial leads
- Upsloping ST segment depression > 1mm at the J point in the precordial leads
- Absence of ST elevation in the precordial leads
- Reciprocal ST segment elevation (0.5mm – 1mm) in aVR
- Typical STEMI morphology may precede or follow the De Winter pattern
Original reports of the de Winter pattern suggested that the ECG did not change or evolve until the culprit artery had been opened. Since then, cases have been reported where the de Winter pattern evolved from, or evolved to, a “classic” anterior STEMI.
Clinical Significance of de Winter T Waves
- The de Winter pattern is seen in ~2% of acute LAD occlusions and is often under-recognised by clinicians
- Key diagnostic features include ST depression and peaked T waves in the precordial leads
- Unfamiliarity with this high-risk ECG pattern may lead to delays in appropriate treatment (e.g. failure of cath lab activation), with attendant negative effects on morbidity and mortality
Background
1947 – The de Winter ECG pattern was first reported by William Dressler (1890-1969) in a study including “Twenty-seven instances of myocardial infarction were studied, in which the first electrocardiogram was taken as early as one and one-quarter hours, and not later than twelve hours, after the onset of symptoms.”
In five cases (18%), high T waves were not associated with abnormal elevation of S-T, nor with significant changes in QRS. Thus, they represented the leading diagnostic sign in the early stage of myocardial infarction.
Dressler, Roesler 1947
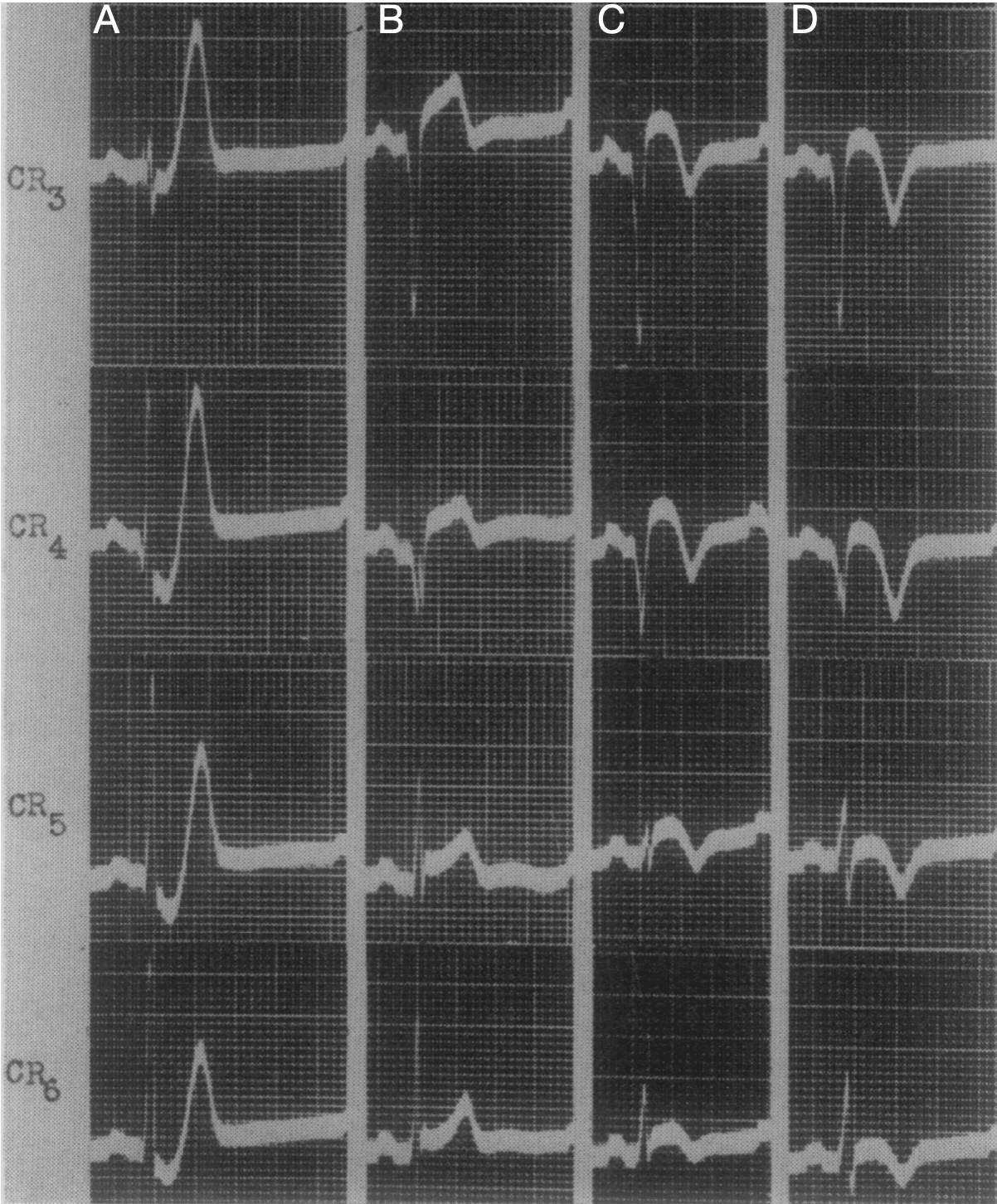
Fig. 3; case 4. Signs diagnostic of anteroseptal infarction. Dressler, Roesler 1947
A: 3 hours after the onset of the attack, shows high T waves in the chest leads associated with abnormal depression of S-T; especially Leads CR3-CR6.
B: 18 hours post symptom onset. Significant changes in QRS appeared when the high T waves had decreased in amplitude and become semi-inverted.
C: 3 days post onset; and D: 7 days post onset, show progressive inversion of the previously high T waves.
2008 – The de Winter ECG pattern was first reported in a case series by de Winter RJ, Verouden NJ, Wellens HJ et al. They observed this ECG pattern in 30 / 1532 patients with acute LAD occlusions (2% of cases)
2009 – Verounden and colleagues replicated this finding in a further case series. They found a de Winter ECG pattern in 35 / 1890 patients requiring PCI to the LAD (2% of cases). Patients with the de Winter ECG pattern were younger, more likely to be male and with a higher incidence of hypercholesterolaemia compared to patients with a classic STEMI pattern
In patients presenting with chest pain, ST-segment depression at the J-point with upsloping ST-segments and tall, symmetrical T-waves in the precordial leads of the 12-lead ECG signifies proximal LAD artery occlusion. It is important for cardiologists and emergency care physicians to recognise this distinct ECG pattern, so they can triage such patients for immediate reperfusion therapy
Verouden NJ 2009

The de Winter ECG pattern is now considered a “STEMI-equivalent” and an indication for immediate reperfusion therapy in many acute coronary syndrome guidelines
Example ECGs
Example 1

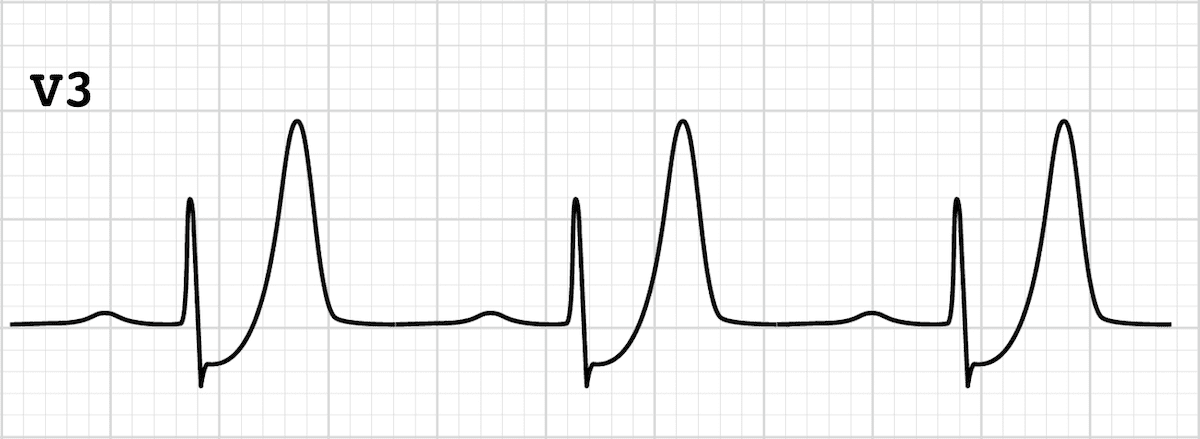
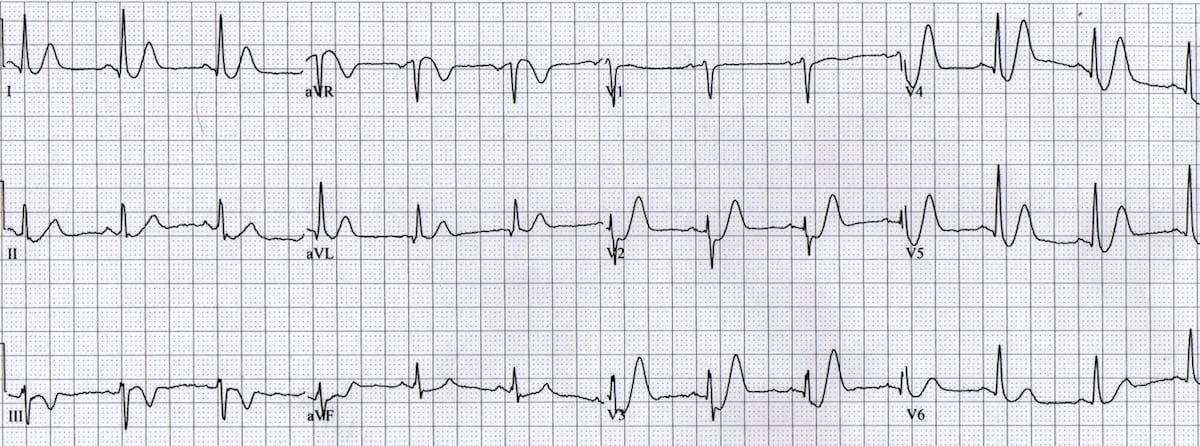
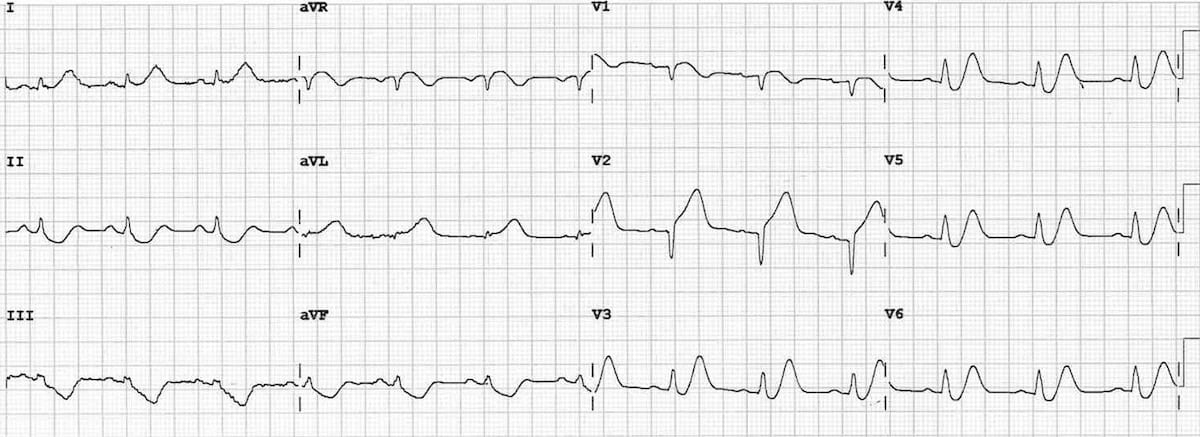
De Winter T waves
- Upsloping ST depression in the precordial leads (> 1mm at J point)
- Peaked anterior T waves (V2-6), with the ascending limb of the T wave commencing below the isoelectric baseline
- Subtle ST elevation in aVR > 0.5mm
There is also some high lateral involvement, with subtle ST elevation in aVL plus reciprocal change in III + aVF. This is consistent with LAD occlusion occurring proximal to the first diagonal branch.
Example 2
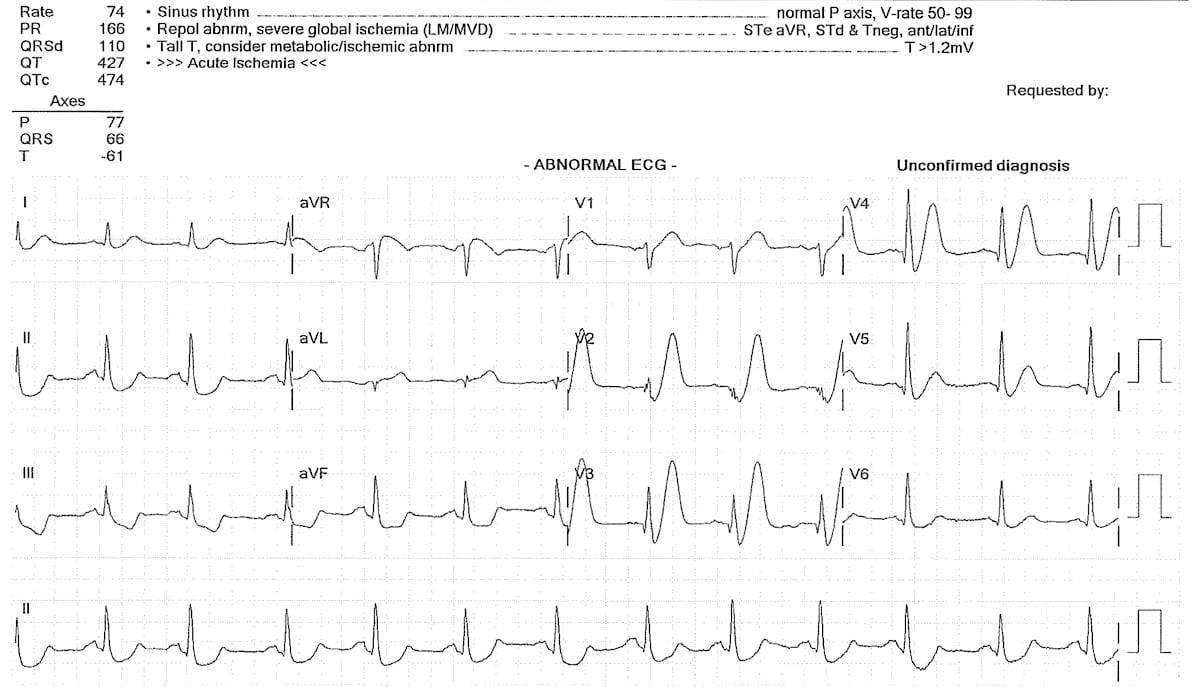
De Winter T waves
- Upsloping ST depression in the precordial leads (> 1mm at J point)
- Peaked anterior T waves (V2-6), with the ascending limb of the T wave commencing below the isoelectric baseline
- Subtle ST elevation in aVR > 0.5mm
Example 3
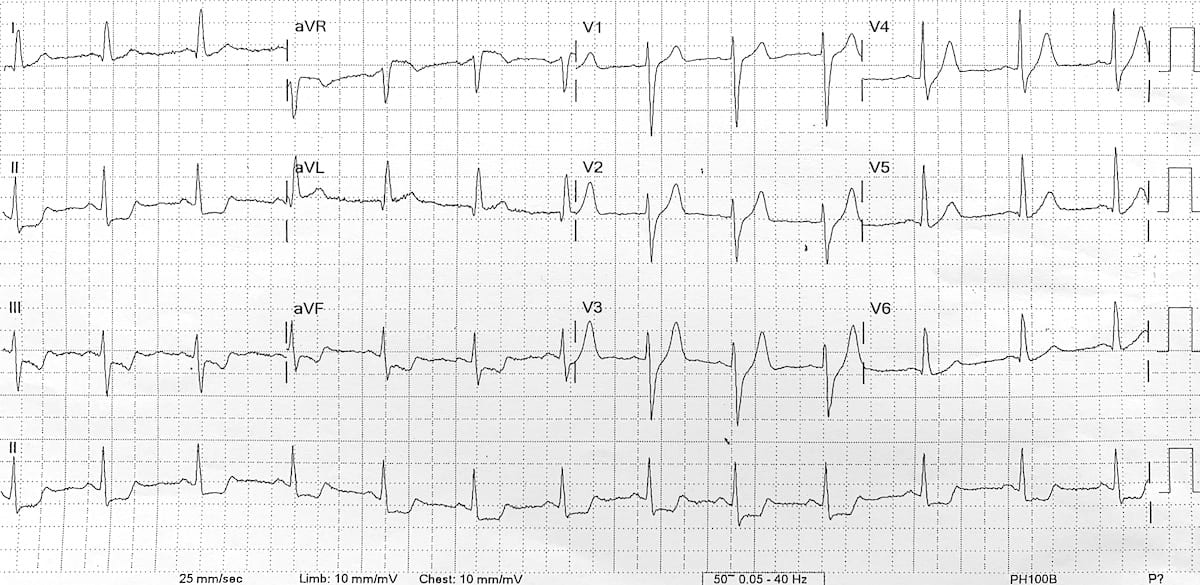
De Winter T waves
- Upsloping ST depression (> 1mm at J point) in the precordial leads V2-6, plus leads I and II
- Peaked anterior T waves, with the ascending limb of the T wave commencing below the isoelectric baseline
- ST elevation in aVR > 0.5mm
Thanks to Dr Steve Smith for contributing this De Winter’s T wave ECG
Example 4
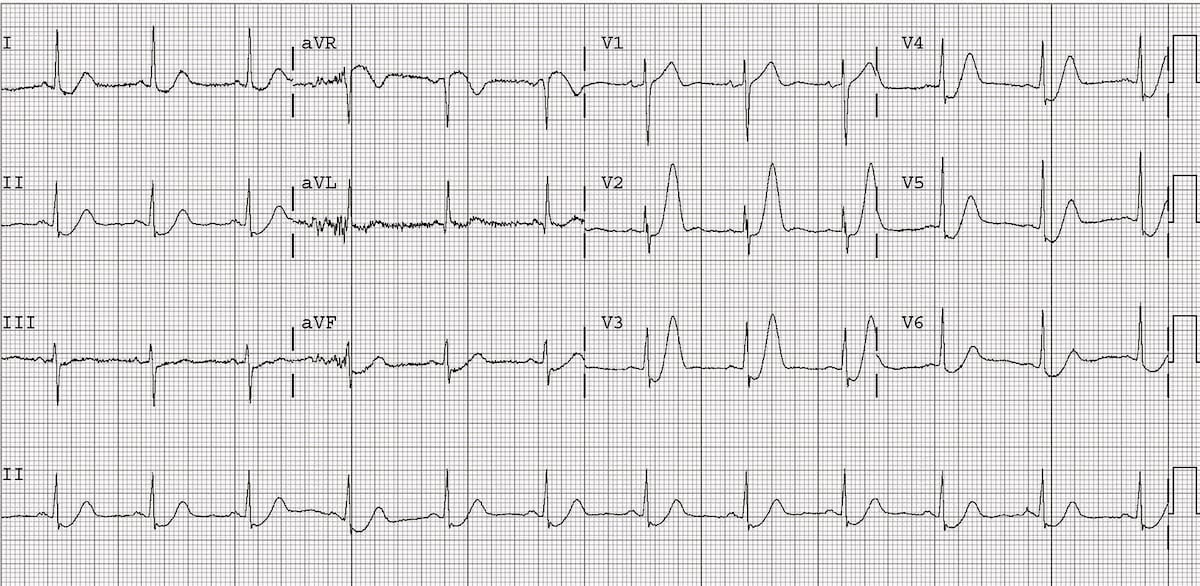
De Winter T waves (morphing into Anterior STEMI)
This great ECG demonstrates de Winter’s T waves combined with features of anterior STEMI — the patient ultimately turned out to have an acute proximal LAD occlusion.
- Upsloping ST depression and peaked T waves (De Winter’s T waves) in V3-6.
- ST elevation in the septal (V1-2) and high lateral leads (I & aVL) with inferior reciprocal change, consistent with an LAD occlusion proximal to the first diagonal branch.
Thanks to Jennifer Davidson for contributing this ECG.
Example 5
Example 6
Cases
- TOP 100 ECG – Case 085
- Smith S. Back pain radiating to the chest in a man in his 40’s
- Smith S. Spontaneous Reperfusion and Re-occlusion
References
de Winter RJ, Verouden NJ, Wellens HJ, Wilde AA. A new ECG sign of proximal LAD occlusion. N Engl J Med. 2008 Nov 6;359(19):2071-3
- Engelen DJ, Gorgels AP, Cheriex EC, De Muinck ED, Ophuis AJ, Dassen WR, Vainer J, van Ommen VG, Wellens HJ. Value of the electrocardiogram in localizing the occlusion site in the left anterior descending coronary artery in acute anterior myocardial infarction. J Am Coll Cardiol. 1999 Aug;34(2):389-95
- Li RA, Leppo M, Miki T, Seino S, Marbán E. Molecular basis of electrocardiographic ST-segment elevation. Circ Res. 2000 Nov 10;87(10):837-9
- Zimetbaum PJ , Josephson ME. Use of the electrocardiogram in acute myocardial infarction. N Engl J Med. 2003 Mar 6;348(10):933-40
- Wang K, Asinger RW, Marriott HJ. ST-segment elevation in conditions other than acute myocardial infarction. N Engl J Med. 2003 Nov 27;349(22):2128-35
- Verouden NJ, Koch KT, Peters RJ, Henriques JP, Baan J, van der Schaaf RJ, Vis MM, Tijssen JG, Piek JJ, Wellens HJ, Wilde AA, de Winter RJ. Persistent precordial “hyperacute” T-waves signify proximal left anterior descending artery occlusion. Heart. 2009 Oct;95(20):1701-6
- NSW Health. Pathway for Acute Coronary Syndrome Assessment (PACSA). Agency for Clinical Innovation. October 2019.
- Eponymythology. History of the Electrocardiogram. LITFL
- Cadogan M. de Winter wave, Eponym A Day. Instagram
- Cadogan M. . Robbert de Winter. LITFL
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
[cite]
ECG LIBRARY
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.

Timing is crazy on this update. Was recently making a lecture on uncommon EKGs not to miss (wellen, sgarbossa, brugada, de Winter. The only one I’ve never had was de Winter. 2 days ago finally got what looked like a real de Winter EKG. Today this update shows up on my email. Had just read the previous update a couple weeks ago so that refresher helped with recognizing that case. Thanks!