
![]()
Ventricular Tachycardia – Monomorphic VT
Ventricular Tachycardia (VT) is a broad complex tachycardia originating from the ventricles. There are several different forms of VT — the most common is monomorphic VT, which originates from a single focus within the ventricles.
ECG features of monomorphic VT
- Regular, broad complex tachycardia
- Uniform QRS complexes within each lead — each QRS is identical (except for fusion/capture beats)

Monomorphic VT can be difficult to differentiate from other causes of broad complex tachycardia.
Other ECG features suggestive of VT include:
- Very broad complexes (>160ms)
- Absence of typical RBBB or LBBB morphology
- Extreme axis deviation (“northwest axis”)
- AV dissociation (P and QRS complexes at different rates)
- Capture beats — occur when the sinoatrial node transiently ‘captures’ the ventricles, in the midst of AV dissociation, to produce a QRS complex of normal duration
- Fusion beats — occur when a sinus and ventricular beat coincide to produce a hybrid complex of intermediate morphology
- Positive or negative concordance throughout the chest leads, i.e. leads V1-6 show entirely positive (R) or entirely negative (QS) complexes, with no RS complexes seen
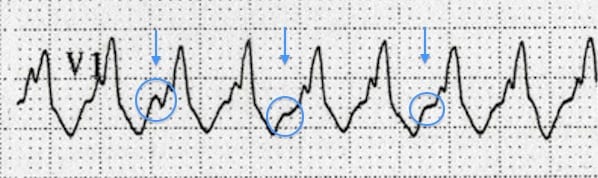
- Josephson’s sign – Notching near the nadir of the S-wave
- Brugada’s sign – The distance from the onset of the QRS complex to the nadir of the S-wave is > 100ms
- RSR’ complexes with a taller “left rabbit ear”. This is the most specific finding in favour of VT. This is in contrast to RBBB, where the right rabbit ear is taller
Below are some examples of positive and negative concordance, and Brugada’s and Josephson’s sign. For more examples of the other suggestive features, see VT versus SVT.
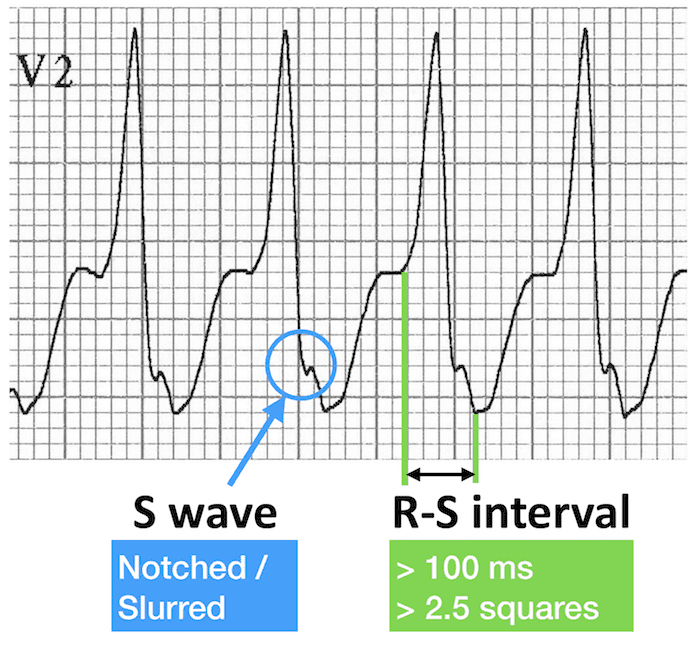
Brugada’s sign (right): R-S interval > 100 ms
Causes of Monomorphic VT
Clinical Significance
- VT may impair cardiac output with consequent hypotension, collapse, and acute cardiac failure. This is due to extreme heart rates and loss of coordinated atrial contraction (“atrial kick”)
- The presence of pre-existing poor ventricular function is strongly associated with cardiovascular compromise
- Decreased cardiac output may result in decreased myocardial perfusion with degeneration into VF
- Prompt recognition and initiation of treatment (e.g. electrical cardioversion) is required in all cases of VT
Ventricular Tachycardia Classification is based on:
1. Clinical Presentation
- Haemodynamically stable
- Haemodynamically unstable — e.g hypotension, chest pain, cardiac failure, decreased conscious level
This is the most important classification clinically and influences immediate management.
2. Duration
- Sustained = Duration > 30 seconds, or requiring intervention due to haemodynamic compromise
- Non-sustained = Three or more consecutive ventricular complexes, terminating spontaneously in < 30 seconds
3. Morphology
- Monomorphic
- Polymorphic VT
- Torsades De Pointes (Polymorphic with QT prolongation)
- Right Ventricular Outflow Tract Tachycardia
- Fascicular Tachycardia
- Bidirectional VT
- Ventricular Flutter
- Ventricular Fibrillation (VF)
Mechanisms of Ventricular Tachycardia
Three mechanisms exist for initiation and propagation of ventricular tachycardia:
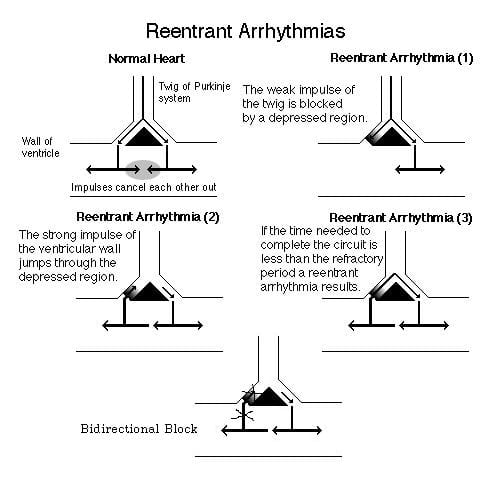
1. Reentry (commonest mechanism)
- Requires two distinct conduction pathways
- Under normal circumstances, impulses cancel each other out (0)
- Conduction block in one pathway develops due to myocardial scarring, usually as a result of prior ischaemia/infarction (1)
- Strong ventricular impulses from the normal/slowed pathway can re-enter the blocked region (2), creating a re-entry circuit (3)
2. Triggered Activity
- Occurs due to early or late after-depolarisations
- Examples include Torsades de Pointes and digitalis toxicity
3. Abnormal Automaticity
- Accelerated abnormal impulse generation by a region of ventricular cells
ECG Examples – Monomorphic VT
Example 1
Monomorphic VT:
- Classic monomorphic VT with uniform QRS complexes
- Indeterminate axis
- Very broad QRS (~200 ms)
- Notching near the nadir of the S wave in lead III = Josephson’s sign
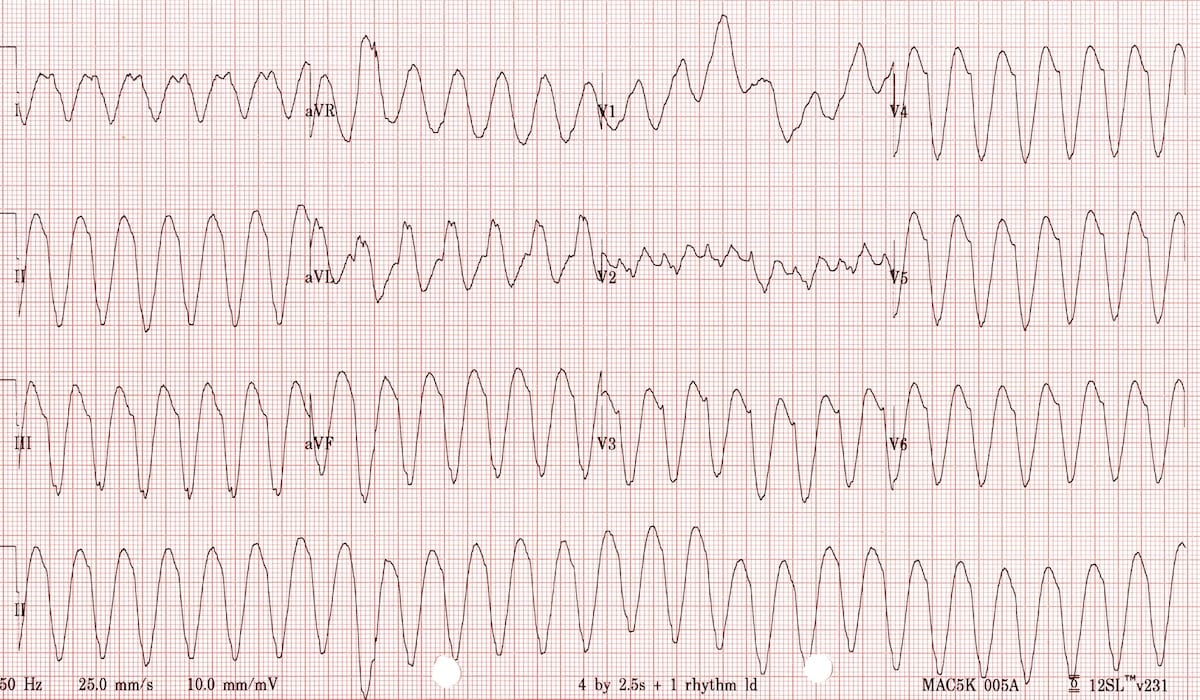
Example 2

Monomorphic VT:
- Very broad QRS complexes (~ 200 ms) with uniform morphology
- Fusion and capture beats are seen in the rhythm strip
- Brugada’s sign is present: the time from the onset of the QRS complex to nadir of S wave is > 100 ms (best seen in V6)
NB: The rhythm strip is recorded after the other 12 leads rather than simultaneously
Example 3

Monomorphic VT:
- Very broad complexes (~ 200 ms in V5-6)
- Northwest axis (-120 degrees)
- Brugada’s sign — the distance from the onset of the QRS complex to the nadir of the S-wave is > 100ms
- Josephson’s sign — notching near the nadir of the S wave is seen in leads II, III, aVF
- Possibly some superimposed P waves in aVF
Example 4
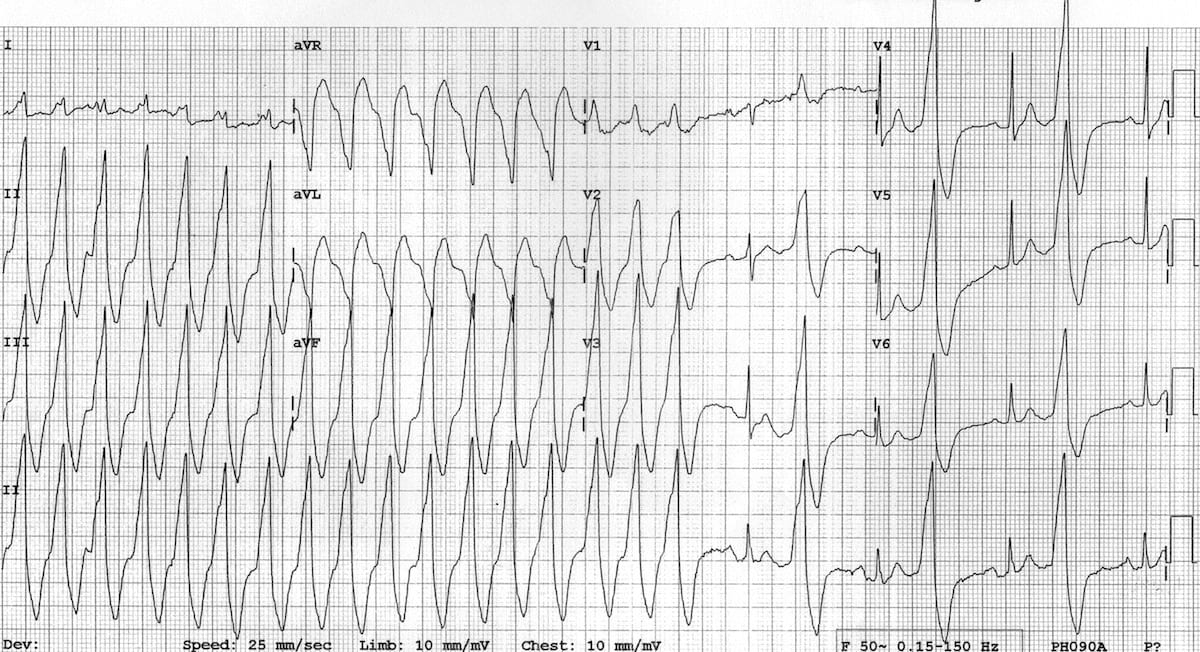
Monomorphic VT alternating with ventricular bigeminy.
The ventricular complexes have the following features:
- Very broad QRS duration (> 160 bpm)
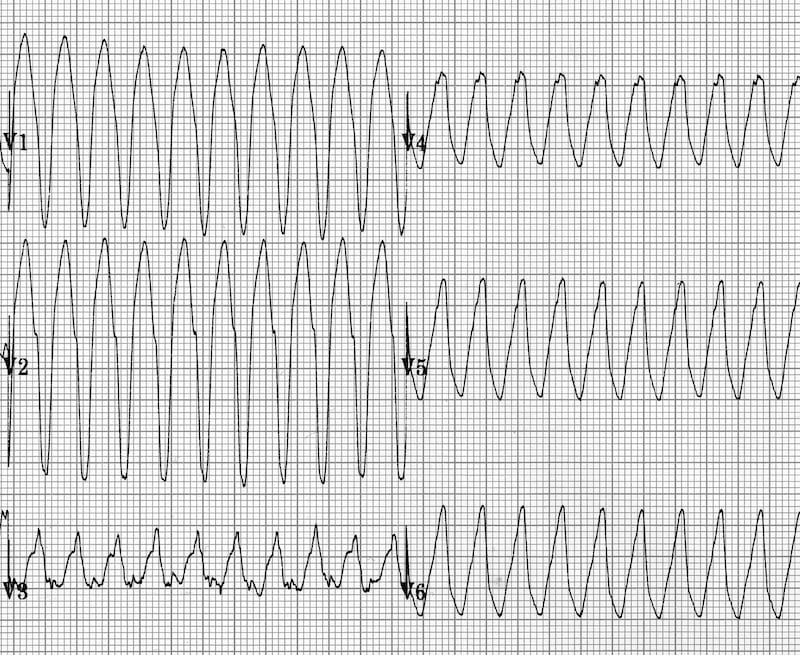
- Positive concordance in the precordial leads (dominant R waves in V1-6)
- Brugada’s sign – time from onset of QRS to nadir of S wave > 100 ms; best seen in leads aVR and aVL
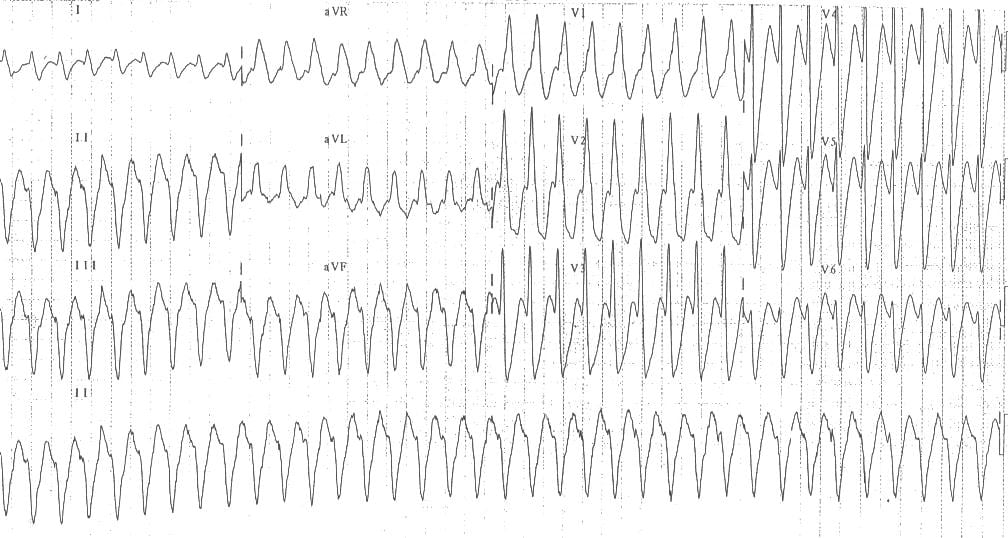
Example 5

Monomorphic VT:
- Extreme axis deviation / northwest axis is present
- -150 degree; QRS positive in aVR, negative in I + aVF
- There is a RBBB-like pattern in V1 with a taller left rabbit ear – this is very specific for VT
Example 6
Monomorphic VT:
- Northwest axis
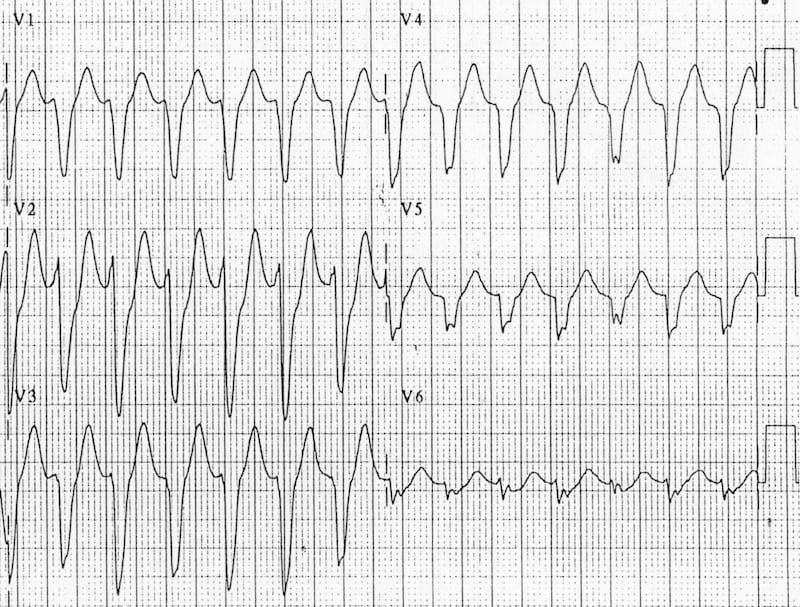
- Tall monophasic R wave in V1 with an rS complex in V6 (small R wave, big S wave) — this pattern is also very specific for VT
This ECG fulfils the Brugada Morphology Criteria for VT.
NOTE: in the presence of a dominant R wave in V1 (“RBBB morphology”), VT is diagnosed if:
- There is an RSR’ complex with a taller left rabbit ear
- There is a tall monophasic R wave
- There is an rS complex in V6 (R/S ratio < 1)
See “VT versus SVT with aberrancy” for more details.
Example 7
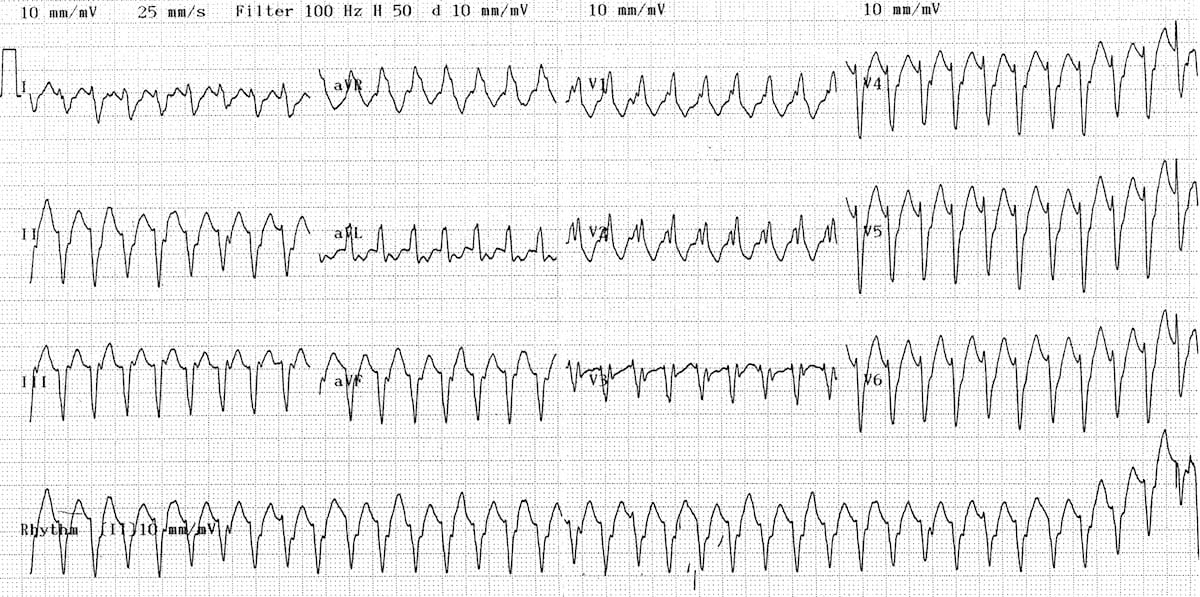
Monomorphic VT:
- This ECG is a difficult one!
- Although there is a broad complex tachycardia (HR > 100, QRS > 120), the appearance in V1 is more suggestive of SVT with aberrancy, given that the the complexes are not that broad (< 160 ms) and the right rabbit ear is taller than the left
- However, on closer inspection there are signs of AV dissociation, with superimposed P waves visible in V1
- Also, the presence of a northwest axis and an rS complex in V6 (tiny R wave, deep S wave) indicate that this is VT
Differential Diagnosis of Wide-Complex Tachycardia
Several arrhythmias can present as a wide-complex tachycardia (QRS > 120 ms), including:
- Ventricular Tachycardia
- SVT with aberrant conduction due to bundle branch block
- SVT with aberrant conduction due to the pre-excitation syndromes
- Pace-maker mediated tachycardia
- Metabolic derangements e.g. hyperkalaemia
- Poisoning with sodium-channel blocking agents (e.g. tricyclic antidepressants)
Differentiating between the various causes of wide-complex tachycardia is challenging and not always possible.
Clinical Features Suggestive of VT
- Age > 35 (positive predictive value of 85%)
- Structural heart disease
- Ischaemic heart disease
- Previous MI
- Congestive heart failure
- Cardiomyopathy
- Family history of sudden cardiac death (suggesting conditions such as HOCM, congenital long QT syndrome, Brugada syndrome or arrhythmogenic right ventricular dysplasia that are associated with episodes of VT)
Diagnostic Algorithms
- A number of diagnostic algorithms exist to help aid in the diagnosis of VT.
- No algorithm is 100% accurate in predicating VT
- Algorithms can be complex and require specific and unfamiliar measurements to be calculated
- Flow charts for the four commonly used algorithms (ACC, Brugada, Ultra-simple Brugada, Vereckei ) can be found over at ECGpedia.org.
Remember
- If in doubt, treat as VT!
Related Topics
Read more about the different types of VT by following these links:
- VT versus SVT with aberrancy
- Right Ventricular Outflow Tract Tachycardia
- Polymorphic VT / Torsades De Pointes
- Fascicular VT
- Bidirectional VT
- Ventricular Flutter
- ECG Exigency 004 – a case of broad complex tachycardia.
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner
[…] E. (2019) Ventricular Tachycardia, Life in The Fast Lane. Available at: https://litfl.com/ventricular-tachycardia-monomorphic-ecg-library/ (Accessed: 28 October […]
Hi Ed,
There was interesting discussion points by Amal on ecgweekly re; rabbit ears this week in diffrentiating SVT and VT
Important to know about, but important to remember “suggestive” doesn’t mean that any or many of these features are a good thing to hang our hats on in terms of ruling “out” VT was my take home?
Thank you for this page on VT.
Regards from CA.
Thanks for all the work you. You have very helpful material. From Ethiopia