
![]()
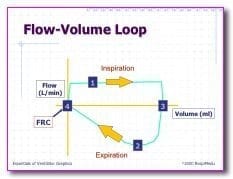
Flow Volume Loops
OVERVIEW
- provide a graphical analysis of inspiratory and expiratory flow from various inspired lung volumes
- breathing across a pneumotachograph subjects inhale to TLC -> FEC manoeuvre -> rapidly inhale back to TLC.
- airflow from TLC is maximal at the beginning of forced exhalation where:
- elastic traction of alveolar septa on airway is greatest
- expiratory muscle strength is greatest
- airway resistance is lowest
- airway resistance increases as forced expiration proceeds due to progressive reduction in airway calibre and is maximal at RV (effort independent part of curve – flow limited by dynamic compression)
- circular in spontaneously breathing patients
- squared but set at an angle in PC and PS breaths
Information Gathered
- peak inspiratory flow rate
- peak expiratory flow rate
- tidal volume
- type of lung and airway pathology
- leaks or air trapping
- water or secretions in circuit
COMMON ABNORMALITIES
Flow limitation can arise from 3 factors:
(1) decreased maximal static expiratory pressure (neuromuscular disease)
(2) increased airway resistance (asthma)
(3) decreased lung elastic recoil pressure (emphysema)
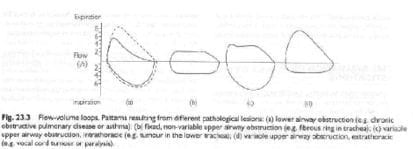
A = lower airway obstruction (COPD/asthma)
B = fixed upper airway obstruction (tracheal stenosis)
C = variable intrathoracic upper airway obstruction (tumour in lower trachea)
D = variable extrathoracic upper airway obstruction (vocal cord tumour or paralysis, enlarge thyroid)
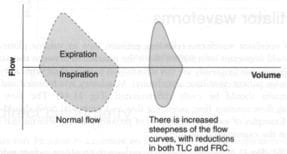
- restrictive lung disease (pulmonary fibrosis)
Leaks or Air Trapping
- loop will not meet at left side where inspiration and expiration end
Jagged Loop
- water of secretion build up
References and Links
CCC Ventilation Series
Modes: Adaptive Support Ventilation (ASV), Airway Pressure Release Ventilation (APRV), High Frequency Oscillation Ventilation (HFOV), High Frequency Ventilation (HFV), Modes of ventilation, Non-Invasive Ventilation (NIV), Spontaneous breathing and mechanical ventilation
Conditions: Acute Respiratory Distress Syndrome (ARDS), ARDS Definitions, ARDS Literature Summaries, Asthma, Bronchopleural Fistula, Burns, Oxygenation and Ventilation, COPD, Haemoptysis, Improving Oxygenation in ARDS, NIV and Asthma, NIV and the Critically Ill, Ventilator Induced Lung Injury (VILI), Volutrauma
Strategies: ARDSnet Ventilation, Open lung approach, Oxygen Saturation Targets, Protective Lung Ventilation, Recruitment manoeuvres in ARDS, Sedation pauses, Selective Lung Ventilation
Adjuncts: Adjunctive Respiratory Therapies, ECMO Overview, Heliox, Neuromuscular blockade in ARDS, Prone positioning and Mechanical Ventilation
Situations: Cuff leak, Difficulty weaning, High Airway Pressures, Post-Intubation Care, Post-intubation hypoxia
Troubleshooting: Autotriggering of the ventilator, High airway and alveolar pressures / pressure alarm, Ventilator Dyssynchrony
Investigation / Indices: A-a gradient, Capnography and waveforms, Electrical Impedance Tomography, Indices that predict difficult weaning, PaO2/FiO2 Ratio (PF), Transpulmonary pressure (TPP)
Extubation: Cuff Leak Test, Extubation Assessment in ED, Extubation Assessment in ICU, NIV for weaning, Post-Extubation Stridor, Spontaneous breathing trial, Unplanned extubation, Weaning from mechanical ventilation
Core Knowledge: Basics of Mechanical Ventilation, Driving Pressure, Dynamic pressure-volume loops, flow versus time graph, flow volume loops, Indications and complications, Intrinsic PEEP (autoPEEP), Oxygen Haemoglobin Dissociation Curve, Positive End Expiratory Pressure (PEEP), Pulmonary Mechanics, Pressure Vs Time Graph, Pressure vs Volume Loop, Setting up a ventilator, Ventilator waveform analysis, Volume vs time graph
Equipment: Capnography and CO2 Detector, Heat and Moisture Exchanger (HME), Ideal helicopter ventilator, Wet Circuit
MISC: Sedation in ICU, Ventilation literature summaries
Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
