
![]()
Appendicitis – the eponymous examination
Eponymythology: The myths behind the history
Eponymous clinical signs in appendicitis and chronic appendicitis. Authors eponymously associated with abdominal signs, symptoms, investigation and management of appendicitis.
appendicitis: appendix (small outgrowth of an internal organ) + -itis (inflammation)
American physician Reginald Heber Fitz (1843–1913) coined the term appendicitis in 1886 when he recognised that the abscesses frequently seen in the right iliac fossa were caused by perforating inflammation of the vermiform (worm-like) appendix. He analysed 466 cases of abdominal disorders that had previously been variously diagnosed and showed that they all involved a diseased appendix.
As a circumscribed peritonitis is simply one event, although usually the most important, in the history of inflammation of the appendix, it seems preferable to use the term appendicitis to express the primary condition.
Fitz 1886
Clinical Signs in Appendicitis
[hide]
- Eponymythology: The myths behind the history
- Aaron sign
- Alders sign
- Arapov Contracture
- Bassler sign
- Bastedo sign
- Blumberg sign
- Bryan Sign
- Cope obturator test
- Cope psoas test
- Dunphy sign
- Lockwood sign
- Markle Sign
- Massouh sign
- McBurney’s point
- Murphy’s Triad
- Perman sign
- Rovsing sign
- Sherren triangle
- Sitkovskiy sign
- Volkovich-Kocher sign
- Voskresensky sign
- References
Alvarado score
Alvarado score for predicting acute appendicitis. In 1986, the American general surgeon Alfredo Alvarado published a retrospective single center study in Philadelphia. His method relies on a combination of factors derived from physical signs, symptoms, and laboratory tests and produces a numerical score used to rule in or rule out acute appendicitis. It is a well-established and widely-used clinical decision tool that may help reduce CT usage.
- Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 1986 May;15(5):557-64
- MDcalc Alvarado Score for Acute Appendicitis is a useful automated tool to record the score
Aaron sign
Aaron sign: Referred pain felt in the epigastrium upon continuous firm pressure over McBurney’s point, indicative of chronic appendicitis
I have been able to induce a referred pain or distress in the epigastrium, left hypochondrium, umbilical, left inguinal or precordial region by a continuous firm pressure over the appendix. I have found this test exceedingly valuable in deciding when and when not to recommend operation for chronic appendicitis
Aaron 1913
- Charles Dettie Aaron (1866 – 1951) American gastroenterologist.
- Aaron CD. A sign indicative of chronic appendicitis. JAMA. 1913; 60(5): 350-351
Alders sign
Alders sign to differentiate the causes of abdominal pain in pregnancy and the puerperium. In a gravid female with a palpable uterus and the patient in a supine position, the examiner locates the site of maximum pain on the abdominal wall. With fingers remaining at this site, turn the patient to the opposite side to a lateral decubitus position. If the pain lessens or disappears, then it is of uterine origin (e.g. leiomyoma, concealed haemorrhage). However, if the pain remains unaltered or fixed then it is deemed to be extrauterine in origin (e.g. appendicitis, ovarian torsion, diverticulitis, or gallbladder disease). Alders referred to this as the “sign of fixed or shifting tenderness”.
With the patient lying straight on her back, the examining fingers find the area of maximum tenderness to pressure on the abdominal wall. While the fingers remain in contact with that area without altering the intensity of pressure they are exerting to elicit pain, the patient is made to turn over on the opposite side so that the plane of the anterior abdominal wall is approximately vertical. The pain produced by the pressure of the fingers will be less or will have entirely disappeared if the lesion is uterine and has fallen away from the examining fingers “shifting tenderness”
Alders 1954: 1194-1195
- Nicholas Alders (1904 – 1995) was a Hungarian born, Austrian trained, English naturalised obstetrician, gynaecologist and surgeon.
- Alders N. Sign for Differentiating Uterine from Extrauterine Complications of Pregnancy and Puerperium. Br Med J. 1951; 2(4741): 1194-5.
Arapov Contracture
Arapov contracture is a reflex contraction of the right hip joint in acute appendicitis. Pain induced reflex contraction of the right hip joint in acute appendicitis
- Dmitry Alekseyevich Arapov (Дмитрий Алексеевич Арапов) (1897 – 1984) Russian military surgeon.
- Arapov DA et al. Paradoxes of acute appendicitis. Vestn. Khir. Im. II Grek. 1968; 101(11): 22-26.
Bassler sign
Bassler sign: Pain induced by compressing (pinching) the appendix between the abdominal wall and iliacus, indicative of chronic appendicitis
When the thumb has been sunk about half-way down to the back of the abdominal cavity, it is swung to the right of the patient at a right angle to the downward pressure line. This pinches the appendix against the iliacus muscle and unyielding structures under and at the side of it, and usually elicits pain or tenderness.
Bassler 1913
- Anthony Bassler (1874 – 1959) American gastroenterologist.
- Bassler A. Pinching the appendix in diagnosis of chronic appendicitis. American Journal of the Medical Sciences. 1913; 146(4): 204-208.
Bastedo sign
Bastedo described a method of dilating the colon with air and causing acute right lower abdominal pain over McBurney’s point to aid in the diagnosis of chronic appendicitis. His original descriptions were presented to the Medical Society of the County of Richmond in 1909
In the routine examination of digestive patients by colon dilation, I noted, some three years ago, that acute pain or tenderness in the region of McBurney’s point on dilation of the colon regularly meant appendicitis.
Bastedo 1910
- Walter Arthur Bastedo (1873 – 1952) was a Canadian-American gastroenterologist
- Bastedo WA. Artificial dilation of stomach and colon as aids in abdominal diagnosis; with a helpful sign in chronic appendicitis. St. Luke’s Hospital Medical and Surgical Reports. 1910; 2: 104-111.
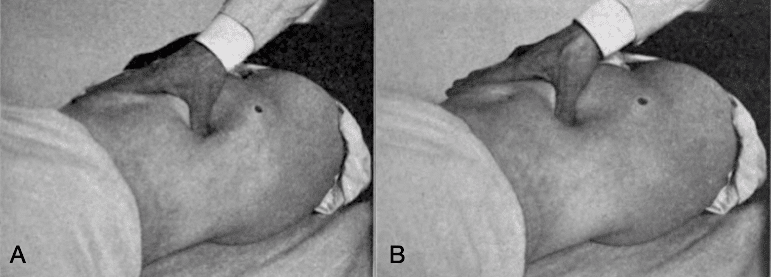
Blumberg sign
Blumberg sign [*aka rebound tenderness ]. Pain felt upon sudden release of steadily applied pressure on the abdomen indicative of peritonitis. Sensitivity 81%; Specificity 49% in diagnosing acute appendicitis.
Performed by gradually increasing the pressure of the palpating hand over the tender spot, and then removing abruptly. If the patient winces with pain upon withdrawal of the hand, the test is positive indicating a likelihood of peritonitis
1907; 54: 1177
{kind=link}
- Jacob Moritz Blumberg (1873 – 1955) German surgeon
- Blumberg, JM. Ueber ein neues diagnostisches Symptom bei Appendicitis. Münchener medizinische Wochenschrift, 1907; 54(1): 1177-1178
Bryan Sign
Bryan presented at the 17th meeting of the South Atlantic Association of Obstetricians and Gynecologists on ‘Surgical Emergencies in Pregnancy and in the Puerperium’. Bryan sign has been shown to have an accuracy rate of 83.8% followed by rebound tenderness (68.6%) in diagnosing appendicitis during pregnancy [Kurtz et al]
In appendicitis, pressure on a pregnant uterus from the left side will often elicit pain in the right lower or middle quadrant.
Bryan 1955: 1205
- Williams McIver Bryan, Jr (1917 – 2007) was an American obstetrician and gynecologist
- Bryan WM Jr. Surgical emergencies in pregnancy and the puerperium. Am J Obstet Gynecol. 1955; 70(6): 1204-1211. discussion, 1211-1213
Cope obturator test
Cope obturator test [*aka thigh-rotation test; obturator test ]. The examiner stands to the right of the patient with the right thigh slightly flexed. The limb is then fully rotated at the hip, first internally and then externally. Positive with conditions causing irritation to the obturator internus muscle e.g. inflammatory fluid in the pelvis, abscess, or perforated appendix. Cope obturator sign: sensitivity (8%); specificity (94%) in diagnosing acute appendicitis.
The right thigh is slightly flexed (so as to relax the psoas muscle) by the surgeon, who stands on the right of the patient: the limb is then fully rotated at the hip, first internally and then externally, so as to put the obturator internus through a full range of movement. The sign is positive if the patient complains of hypogastric pain when the limb is moved in this manner
Cope 1919
- Sir Vincent Zachary Cope (1881 – 1974) English surgeon.
- Cope VZ. The thigh-rotation or obturator test: A new sign in some inflammatory conditions. Br J Surg. 1919; 7: 537.
Cope psoas test
Cope psoas test [*aka Ilio-psoas rigidity; psoas extension test; Obraztsova sign, Симптом Образцова ]. The patient is lying in the lateral decubitus position opposite the side where the pain is located. Extension of the thigh causes pain.May be positive in retrocaecal appendicitis as well as primary/secondary psoas abscess. Cope psoas test: sensitivity (13 – 42%); specificity (79 – 97%); positive likelihood ratio of 2.0 for detecting appendicitis.
It is well known that if there be an inflamed focus in relation to the psoas muscle the corresponding thigh is often flexed by the patient to relieve the pain. A lesser degree of such contraction (and irritation) can be determined often by making the patient lie on the opposite side and extending the thigh on the affected side to the full extent. Pain will be caused by the maneuver if the psoas is rigid from either reflex or direct irritation
Cope 1921
- Sir Vincent Zachary Cope (1881 – 1974) English surgeon.
- Cope Z. Method of diagnosis: (II) The examination of the patient. Determination of illiopsoas rigidity. 1921
Dunphy sign
Dunphy sign [* cough test; coughing test ] increased abdominal pain, localised to the right lower quadrant, with coughing. In 2009 Idris et al published a cohort study of 866 patients with cough test sensitivity (95%) and specificity (80%) for acute appendicitis.
The patient should first be asked to cough. In the presence of acute peritoneal inflammation this usually elicits a sharp twinge of pain localized to the involved area. It is extremely valuable to elicit this “cough tenderness” and have the patient point with one finger to the exact area of pain. This localizes the area of inflammation before the examiner so much as touches the patient
Dunphy 1953
- Most commonly referenced as Osborne Joby Dunphy (1898–1989)…however I can find no records, or publications pertaining to this individual. More probably an eponymous tribute to the eminent American surgeon John Englebert Dunphy (1908-1981)
- Dunphy JE, Botsford TW. Examination of the Abdomen: Acute appendicitis. In: Physical Examination Of The Surgical Patient. 1953: 123-124
Lockwood sign
Lockwood sign first appeared in a letter to the Editors of British Medical Journal. George Herbert Colt (1878-1957) wrote that the late Mr. CB. Lockwood taught his dressers as follows:
The patient lies on his back with his head raised on a pillow and his knees drawn up, so that the superficial abdominal muscles are relaxed. The surgeon sits down near his right side and palpates the right iliac region near McBurney’s spot with the three inner fingers of his left hand. If he feels a trickle of flatulence passing his fingers, and if this can be often repeated after waiting a half to one minute or a little longer, the patient has either a chronically inflamed appendix or adhesions near it.
Colt. 1932
- Charles Barrett Lockwood (1856 – 1914) English surgeon.
- Colt GH. Chronic Appendicitis: “Lockwood’s Sign”. Br Med J. 1932 Nov 19; 2(3750): 942.
Markle Sign
Markle Sign, Markle Test or Heel Drop Jarring Test is elicited in patients with intraperitoneal inflammation by having a patient stand on his or her toes and suddenly dropping down onto the heels with an audible thump. If abdominal pain is localised as the heels strike the ground, the Markle Sign is positive. If the pain is localised to the right lower quadrant, this is suggestive of acute appendicitis.
- George Bushar Markle IV (1921-1999) American surgeon
- Markle, GB. A simple test for intraperitoneal inflammation. The American Journal of Surgery. 1973; 125(6): 721-722
Massouh sign
Massouh sign: A firm swish of the examiner’s index and middle finger across the patient’s abdomen from xiphoid sternum to first the left and then the right iliac fossa. A positive Massouh sign is a grimace of the patient upon a right sided (and not left) sweep.
- Farouk Massouh is a British General Surgeon
- Publication of evidence is limited to a tweet; a Linkedin post; and a wikipedia article:
McBurney’s point
McBurney’s point lies one-third of the distance laterally on a line drawn from the umbilicus to the right anterior superior iliac spine…or as McBurney described it:
The seat of greatest pain, determined by the pressure of one finger, has been very exactly between an inch and a half and two inches from the anterior spinous process of the ilium on a straight line drawn from that process to the umbilicus
McBurney 1889
Classically used as a guide to the location of the base of the appendix, determined by pain elicited by the pressure of a single digit at the point (McBurney’s sign).
Note: Mathematics confuses semantics. McBurney originally described his point at a set distance from a fixed point (ASIS) along a line between two fixed points (ASIS and umbilicus). In recent times this point has been re-defined as fraction (one third) of the distance between the two fixed points (ASIS and umbilicus).
Note: McBurney’s point (1889) and McBurney’s Incision (1894) are not the same.
It has seemed to me that in all cases where it is desirable first to locate the base of the appendix, and usually too where one wishes to make an entrance into an abscess originating in disease of this organ, it is much better to incise the abdominal wall a little to the outer side (lateral) of the normal situation of the appendix
McBurney 1894
- Charles Heber McBurney (1845-1913) American general surgeon
- McBurney C. Experience with early operative interference in cases of disease of the vermiform appendix. New York Medical Journal, 1889; 50: 676-684.
Murphy’s Triad
1895 – Murphy initially presented a quadrad of signs in his report and analysis of one hundred and forty-one histories and laparotomies
Upon what cases should we operate? Upon every case of appendicitis, or better, upon every case where we have present the four cardinal symptoms: 1. Sudden attack of pain over appendix. 2. Always nausea, frequently vomiting. 3. Elevation of temperature, and 4. Local tenderness in the position occupied by the appendix
Murphy 1895
1904 – Murphy recognized an ordered sequence of signs and symptoms in his analysis of Two Thousand Operations for Appendicitis and Deductions from His Personal Experience. He included low grade fever in the sequence but with the proviso that a raised temperature at any given stage of the attack is not invariable and is not an essential feature in establishing a diagnosis. Murphy’s sequence (quadrad) is often shortened to a triad of signs and symptoms excluding fever.
The symptoms in the order of their occurrence may be mentioned as: first, pain in the abdomen, sudden and severe, followed by (second) nausea or vomiting, even within a few hours, most commonly between three and four hours after the onset of pain; third, general abdominal sensitiveness most marked in the right side, or more particularly over the appendix; fourth, elevation of temperature, beginning from two to twenty-four hours after the onset of pain…The symptoms occur almost without exception in the above order, and when that order varies I always question the diagnosis. If the nausea and vomiting or temperature precede the pain I feel certain that the case is not one of appendicitis
Murphy 1904: 190
- John Benjamin Murphy (1857 – 1916) American physician and abdominal surgeon
- Murphy JB. Appendicitis: with original report and analysis of one hundred and forty-one histories and laparotomies for that disease under personal observation. 1895
- Murphy JB. Two Thousand Operations for Appendicitis and Deductions from His Personal Experience. Am J Med Sci 1904; 128: 187–211
Perman sign
In 1904 Emil S Perman briefly described a sign of appendicitis in his article titled “Om indikationerna för operation vid appendicit samt redogörelse for å Sabbatsbergs sjukhus opererade fall“, which involved pain over the ileocaecal tract (right iliac fossa) elicited by applying pressure to the left abdomen (left iliac fossa). Referred to as Perman-Rovsing sign, or incorrectly as Rovsing sign.
Original
English
Därpå har jag äfven alltid funnit ett annat symtom tyda, nämligen en till ileooekaltrakten lokaliserad smärta vid tryck å- vänstra delen af buken.
Perman ES. 1904: 806
Furthermore, I have always found another symptom evident, namely a pain located to the ileoecal tract with pressure to the left part of the abdomen.
Perman ES. 1904: 806
- Emil Samuel Perman (1856 – 1946) was a Swedish general surgeon
- Perman ES. Om indikationerna för operation vid appendicit samt redogörelse for å Sabbatsbergs sjukhus opererade fall [About the indications for surgery in appendicitis and an account of cases at Sabbatsberg Hospital]. Hygiea 1904; 66(2): 797-847
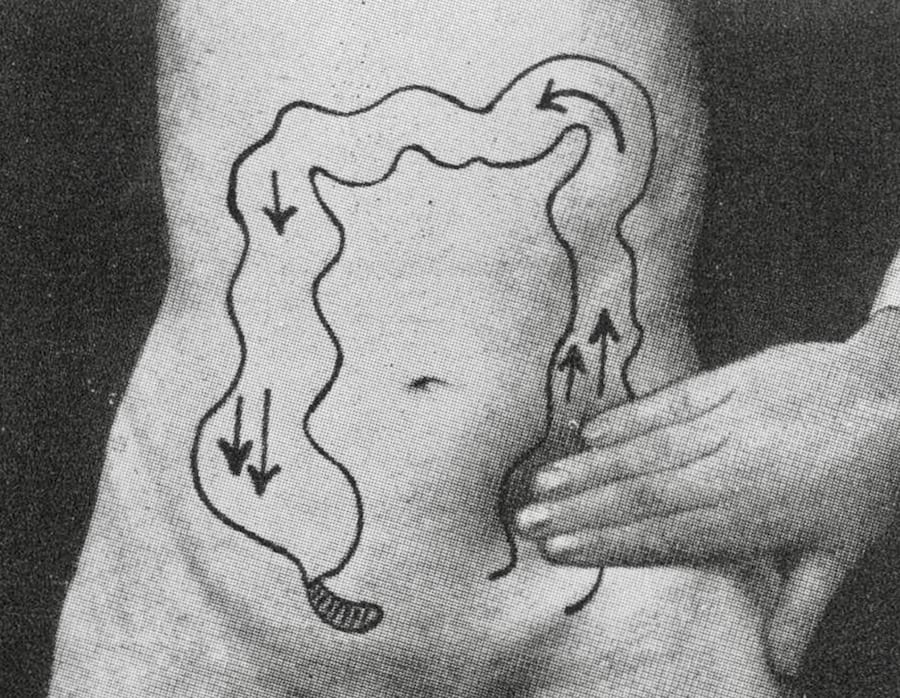
Rovsing sign
Modern interpretation of Rovsing sign: In acute appendicitis, palpation of the left lower quadrant may elicit pain in the right lower quadrant. If this occurs, it is said to be a positive Rovsing sign.
However, the Rovsing sign is described variably in medical literature with most descriptions bearing little/no resemblance to the 1907 description by Rovsing, but rather the description offered by Perman (above) in 1904. Rovsing’s original description and intent were quite different. Rovsing described the manoeuvre as an attempt to distend the caecum and appendix by applying pressure to the left colon, in an anti-peristaltic fashion.
I press with my right hand onto the fingers of the left hand that is lying flat against the colon descendens [descending colon] and then let the hand glide up toward the splenic flexure…The entire method is based upon isolated rise of pressure within the colon.
Rovsing 1907
In doing this correctly, Rovsing suggests that if pain is elicited, then this isolates the source to the caecum or appendix, and rules out other structures in the right iliac fossa.
- Niels Thorkild Rovsing (1862-1927) was a Danish surgeon
- Rovsing T. Indirektes Hervorrufen des typischen Schmerzes an McBurney’s Punkt. Ein Beitrag zur Diagnostik der Appendicitis und Typhlitis [Indirect elicitation of the typical pain at McBurney’s point. A contribution to the diagnosis of appendicitis and typhlitis]. Zentralblatt für Chirurgie 1907;34:1257-59
Sherren triangle
Sherren triangle is formed by the lines joining the summit of the iliac crest, the pubic tubercle and umbilicus. Sherren proposed the skin of this triangle is hyperaesthetic found in acute appendicitis
Cutaneous hyperalgesia is tested by gently pinching or stroking the skin, beginning if possible in an area which is not tender and working towards the suspected tender area and so marking out its boundaries…As an aid in determining operation the disappearance of hyperalgesia is of the utmost importance. If well-marked superficial tenderness disappears without coincident amelioration of the general condition of the patient it is a sign of perforation or gangrene of the appendix.
Sherren 1903
- James Sherren (1872 – 1945) British General surgeon
- Sherren J. On the occurrence and significance of cutaneous hyperalgesia in appendicitis. Lancet 1903; 162(4177): 816-821
- Sherren J. The causation and treatment of Appendicitis. Practitioner, 1905; 74: 833-844
Sitkovskiy sign
Sitkovskiy sign [*aka Rosenstein Sign ]. Tenderness in the right lower quadrant increases when the patient moves from the supine position to a recumbent posture on the left side
- Piotr Porfiryevich Sitkovskiy (Петр Порфирьевич Ситковский) (1882 – 1933) Russian surgeon.
- Paul Rosenstein (1875 – 1964) German urologist
- Ситковский П. П. Об одном из клинических признаков при воспалении червеобразного отростка, Туркестанск. мед. журн., т. 1, № 1, с. 37, 1922
Volkovich-Kocher sign
The appearance of pain in the epigastric region or around the stomach at the beginning of disease with a subsequent shift to the right iliac region.
- Nikolay Markianovich Volkovich (Николай Маркианович Волкович) (1858 – 1928) Ukrainian surgeon.
- Волкович Н. М. Аппендицит, желчно-каменная болезнь, туберкулезный перитонит – Киев, 1926.
Voskresensky sign
Voskresensky symptom (симптом Воскресенского) Clinical sign of appendicitis with low sensitivity and specificity, found in 36.8% of patients with uncomplicated appendicitis and 33.5% with gangrenous appendicitis.
Original
English
Тест проводится экзаменатором, который тянет левую руку за нижний край рубашки пациента и помещает кончики пальцев второй / четвертой правой руки на брюшную стенку в эпигастрии. Экзаменатор оказывает давление на брюшную полость вниз, перемещая или двигая рукой в направлении правого нижнего квадранта и останавливаясь в этой области. Положительным признаком является то, что пациент сообщает об усилении боли в этой области.
Воскресенский. Советская медицина 1940
The test is performed by the examiner pulling the lower edge of a patient’s shirt with his left hand and places the second through fourth fingertips of his/her right hand on the abdominal wall in the epigastrium. The examiner exerts downward pressure on the abdomen while moving or sliding his hand towards the right lower quadrant and stopping in this region. A positive sign is if the patient reports increasing pain in this region
Voskresensky. Soviet medicine. 1940
- Vladimir Mikhailovich Voskresensky Владимир Михайлович Воскресенский (1902 – 1951) Russian general surgeon
- Новый симптом острого аппендицита (A new symptom of acute appendicitis). Советская медицина. 1940; 10.
Of all the ills within the abdomen
Zachary Cope 1921
Which cause affliction to the sons of men
There’s none more often puts them in a fix
Than trouble in the worm-like appendix
References
- Fitz RH. Perforating inflammation of the vermiform appendix: with special reference to its early diagnosis and treatment. 1886
- Moore SW. The Physiological Basis for Diagnostic Signs of an Acute Abdomen. Surgical Clinics of North America, 1958; 38(2): 371–383.
- Berry J Jr, Malt RA. Appendicitis near its centenary. Ann Surg. 1984; 200(5): 567-75
- Butsenko VN, Antoniuk SM. [Significance of the separate symptoms in acute appendicitis]. Klinicheskaia khirurgiia Klin Khir. 1992;(2):33-5.
- Wagner JM, McKinney WP, Carpenter JL. Does this patient have appendicitis? JAMA. 1996;276(19):1589-94.
- McGee S. Evidence-Based Physical Diagnosis. Elsevier
- Alvarado A. How to improve the clinical diagnosis of acute appendicitis in resource limited settings. World J Emerg Surg. 2016 Apr 26;11:16.
- Rastogi V et al. Abdominal Physical Signs and Medical Eponyms: Movements and Compression. Clin Med Res. 2018; 16(3-4): 76-82
[cite]
eponymictionary
the names behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
