
![]()
Q Wave
The Q Wave
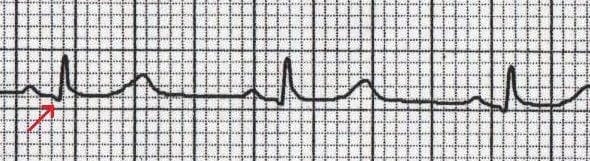
A Q wave is any negative deflection that precedes an R wave
- The Q wave represents the normal left-to-right depolarisation of the interventricular septum
- Small ‘septal’ Q waves are typically seen in the left-sided leads (I, aVL, V5 and V6)
Q waves in context
Q waves in different leads
- Small Q waves are normal in most leads
- Deeper Q waves (>2 mm) may be seen in leads III and aVR as a normal variant
- Under normal circumstances, Q waves are not seen in the right-sided leads (V1-3)
Pathological Q Waves
Q waves are considered pathological if:
- > 40 ms (1 mm) wide
- > 2 mm deep
- > 25% of depth of QRS complex
- Seen in leads V1-3
Pathological Q waves usually indicate current or prior myocardial infarction.
Differential Diagnosis
- Myocardial infarction
- Cardiomyopathies — Hypertrophic (HCM), infiltrative myocardial disease
- Rotation of the heart — Extreme clockwise or counter-clockwise rotation
- Lead placement errors — e.g. upper limb leads placed on lower limbs
Loss of normal Q waves
- The absence of small septal Q waves in leads V5-6 should be considered abnormal.
- Absent Q waves in V5-6 is most commonly due to LBBB.
ECG Examples
Example 1
- Inferior Q waves (II, III, aVF) with ST elevation due to acute MI
Example 2
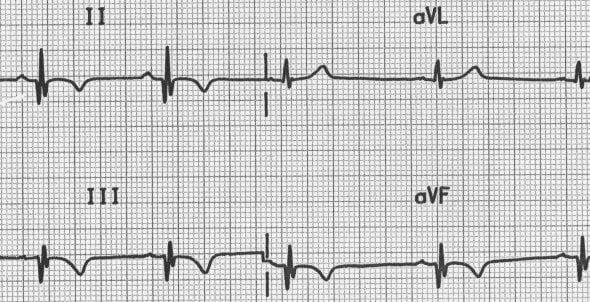
- Inferior Q waves (II, III, aVF) with T-wave inversion due to previous MI
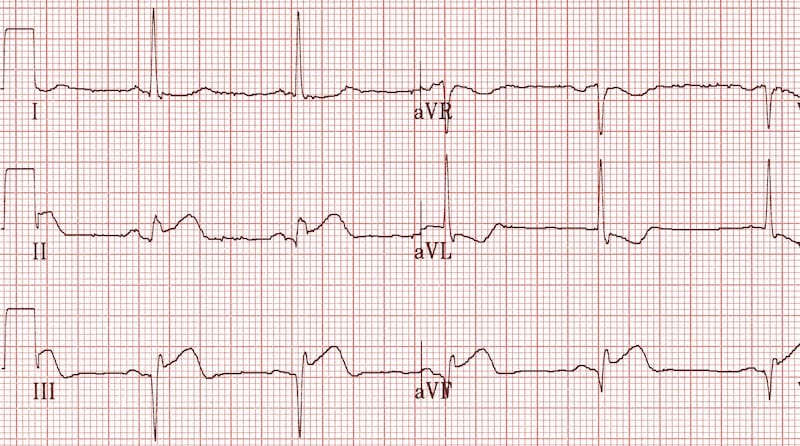
Example 3
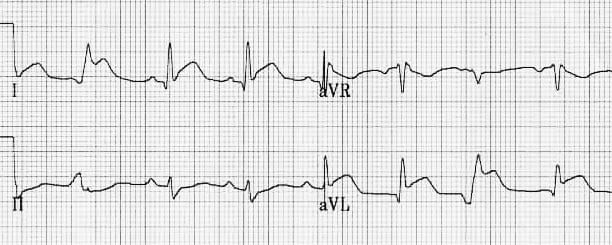
- Lateral Q waves (I, aVL) with ST elevation due to acute MI
Example 4
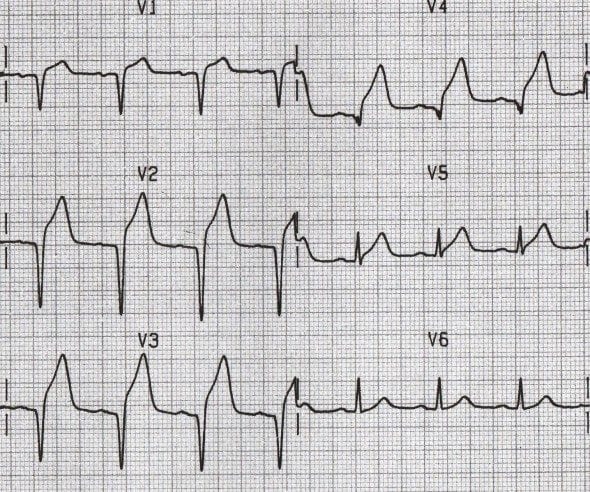
- Anterior Q waves (V1-4) with ST elevation due to acute MI
Example 5
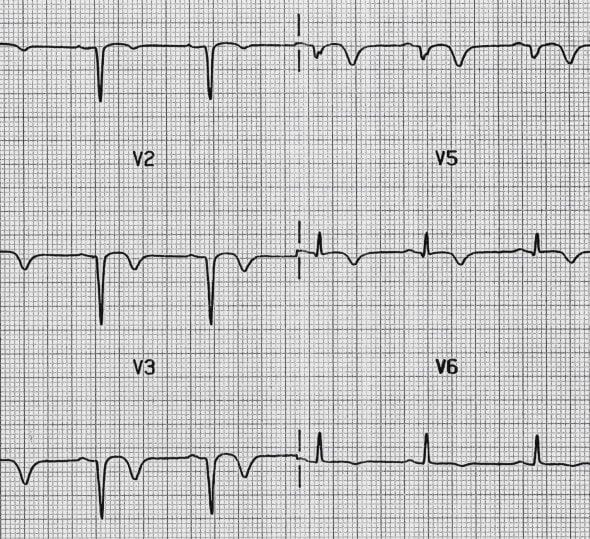
- Anterior Q waves (V1-4) with T-wave inversion due to recent MI
ECG Library Basics
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
Thankyou for this Dr Burns,
I wonder what your thoughts are on finding inferior Q waves in a patient with an indeterminate axis? Should we still expect the small inferior R waves seen in a superior axis?
Thank you for this concise but informative post.
Just a question: would that be safe to say that in example 4 and 5, there are only Q waves in Leads V1 to V4, and no R wave, no S wave, then we are onto ST elevation?
Yes correct. Otherwise known as poor R wave progression, we see complete loss of R waves which is common in acute infarction.
[…] https://litfl.com/q-wave-ecg-library/ […]
Why we considered Q wave and T waves inversion as recent MI in Example 5 but in Example 2 considered as previous?