
![]()
QRS Interval
QRS Complex Morphology
Main features to consider:
- Width of the complexes: Narrow versus broad.
- Voltage (height) of the complexes.
- Spot diagnoses: Specific morphology patterns that are important to recognise.
QRS Complex Naming Convention

QRS Width
Normal QRS width is 70-100 ms (a duration of 110 ms is sometimes observed in healthy subjects). The QRS width is useful in determining the origin of each QRS complex (e.g. sinus, atrial, junctional or ventricular).
- Narrow complexes (QRS < 100 ms) are supraventricular in origin.
- Broad complexes (QRS > 100 ms) may be either ventricular in origin, or due to aberrant conduction of supraventricular complexes (e.g. due to bundle branch block, hyperkalaemia or sodium-channel blockade).

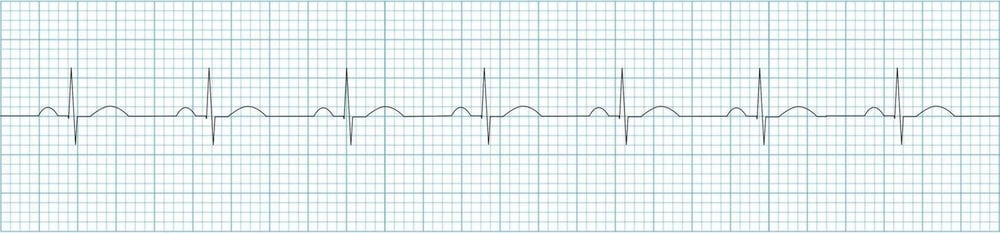
Sinus rhythm with frequent ventricular ectopic beats (VEBs) in a pattern of ventricular bigeminy. The narrow beats are sinus in origin, the broad complexes are ventricular.
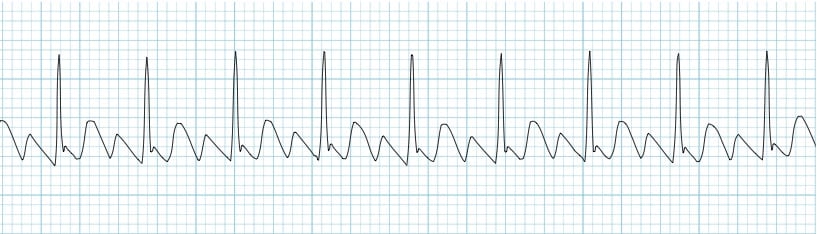
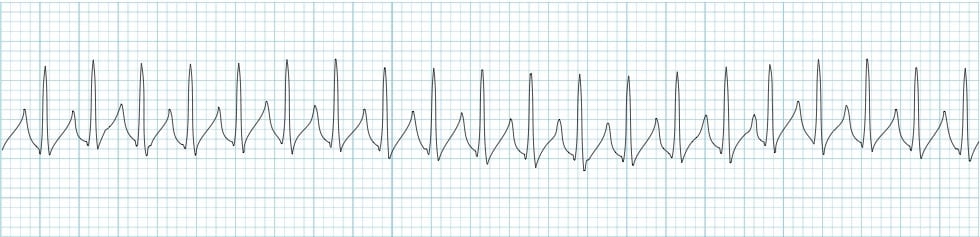
Narrow QRS Complex Morphology
Narrow (supraventricular) complexes arise from three main places:
- Sino-atrial node (= normal P wave)
- Atria (= abnormal P wave / flutter wave / fibrillatory wave)
- AV node / junction (= either no P wave or an abnormal P wave with a PR interval < 120 ms)
Examples of Narrow Complex Rhythms:
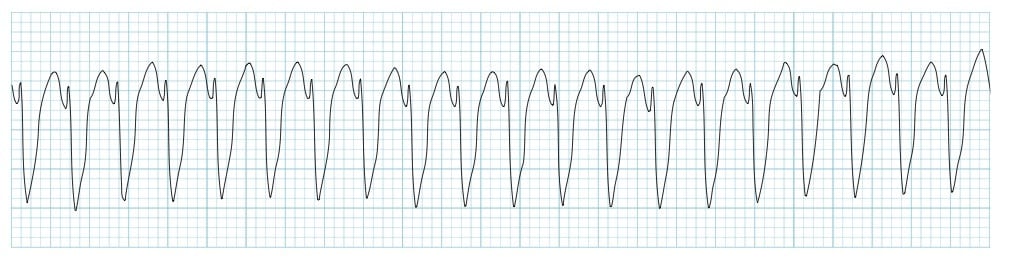
Broad QRS Complex Morphology
Broad/Wide QRS Complexes
- A QRS duration > 100 ms is abnormal
- A QRS duration > 120 ms is required for the diagnosis of bundle branch block or ventricular rhythm
Broad complexes may be ventricular in origin or due to aberrant conduction secondary to:
- Bundle branch block (RBBB or LBBB)
- Hyperkalaemia
- Poisoning with sodium-channel blocking agents (e.g. tricyclic antidepressants)
- Pre-excitation (i.e. Wolff-Parkinson-White syndrome)
- Ventricular pacing
- Hypothermia
- Intermittent aberrancy (e.g. rate-related aberrancy)
Example of a Broad Complex Rhythm:
Ventricular vs supraventricular rhythms
Differentiation between ventricular complexes and aberrantly conducted supraventricular complexes may be difficult.
- In general, aberrant conduction of sinus rhythm and atrial rhythms (tachycardia, flutter, fibrillation) can usually be identified by the presence of preceding atrial activity (P waves, flutter waves, fibrillatory waves).
- However, aberrantly conducted junctional (AV nodal) complexes may appear identical to ventricular complexes as both produce broad QRS without any preceding atrial activity.
- In the case of ectopic beats, this distinction is not really important (as occasional ectopic beats do not usually require treatment).
- However, in the case of sustained tachyarrhythmias, the distinction between ventricular tachycardia and SVT with aberrancy becomes more important. This topic is covered in more detail here.
Fortunately, many causes of broad QRS can be identified by pattern recognition:
- Right bundle branch block produces an RSR’ pattern in V1 and deep slurred S waves in the lateral leads.
- Left bundle branch block produces a dominant S wave in V1 with broad, notched R waves and absent Q waves in the lateral leads.
- Hyperkalaemia is associated with a range of abnormalities including peaked T waves
- Tricyclic poisoning is associated with sinus tachycardia and tall R’ wave in aVR
- Wolff-Parkinson White syndrome is characterised by a short PR interval and delta waves
- Ventricular pacing will usually have visible pacing spikes
- Hypothermia is associated with bradycardia, long QT, Osborn waves and shivering artefact
High Voltage QRS Morphology
- Increased QRS voltage is often taken to infer the presence of left ventricular hypertrophy.
- However, high left ventricular voltage (HLVV) may be a normal finding in patients less than 40-45 years of age, particularly slim or athletic individuals.
- There are multiple “voltage criteria” for left ventricular hypertrophy.
- Probably the most commonly used are the Sokolov-Lyon criteria (S wave depth in V1 + tallest R wave height in V5-V6 > 35 mm).
- Voltage criteria must be accompanied by non-voltage criteria to be considered diagnostic of left ventricular hypertrophy.
Low Voltage QRS Morphology
The QRS is said to be low voltage when:
- The amplitudes of all the QRS complexes in the limb leads are < 5 mm; or
- The amplitudes of all the QRS complexes in the precordial leads are < 10 mm
Electrical Alternans
- This is when the QRS complexes alternate in height.
- The most important cause is massive pericardial effusion, in which the alternating QRS voltage is due to the heart swinging back and forth within a large fluid-filled pericardium.
Spot Diagnoses
These cardiac diseases produce distinctive QRS morphologies that are important not to miss:
- Brugada syndrome (partial RBBB with ST elevation in V1-2)
- Wolff-Parkinson White Syndrome (delta wave)
- Tricyclic poisoning (wide QRS with dominant R wave in aVR)
ECG Library Basics
- P Wave
- PR Interval
- PR Segment
- Q Wave
- QRS Segment
- QT Interval
- J Point
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |