
![]()
Dobutamine
CLASS
- Synthetic catecholamine
- Direct-acting moderately selective β1 adrenergic agonist
- Inotrope
RACEMIC NATURE AND CHEMICAL STRUCTURE
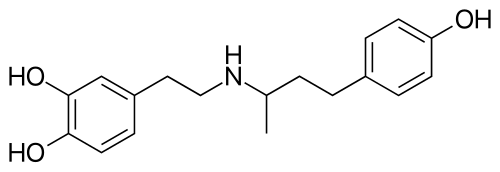
- Racemic Mixture: Dobutamine is a racemic mixture of two stereoisomers: the (+) isomer and the (−) isomer.
- (+) Isomer: Potent β1 agonist (~10x the agonist effect of the (-)isomer), weak β2 agonist, and competitive alpha-1 antagonist.
- (−) Isomer: primarily α1 agonist effect; weak β1 and β2 agonist effect.
- Implications: The racemic nature results in a net effect of potent β1 agonism, weak β2 agonism, and minimal/ weak α1 partial agonism.
- Chemical Structure: The presence of a bulky aryl alkyl substituent group on the amine nitrogen of the phenylethanolamine backbone confers high β1 selectivity by sterically hindering interaction with binding sites on β2 and α receptors.
MECHANISM OF ACTION
- Receptor Interactions: Primarily stimulates β1 adrenergic receptors in the heart, with mild β2 effect. Overall effect is moderately selective b1 agonism (β1 >> β2 > α1).
- Anatomic Locations: Cardiac myocytes.
- Second Messenger Pathways: β1 receptor activation in cardiac myocytes leads to:
- Adenylate cyclase activation -> Increased cAMP Levels -> activation of protein kinase A (PKA) -> phosphorylation of L-type calcium channels, increasing calcium influx into the cells -> further calcium release from the sarcoplasmic reticulum
- Effects of calcium release in cardiac cells:
- Increased contractility
- Increased heart rate due to increased automaticity of SAN pacemaker cells and AVN conduction
- Pharmacodynamic Effects:
- Positive inotropy (contractility)
- Positive lusitropy (relaxation)
- Positive chronotropy (heart rate) – less than isoprenaline (non-selective β agonist)
- Positive dromotropy (conduction velocity)
- Increased oxygen demand (myocardial VO2)
- Increased cardiac output with little change in TPR (weak β2 mediated vasodilation balanced by weak α1 vasoconstriction)
- Decreased LVEDP
- Duration of Effect:
- Rapid onset within 1-2 minutes, peak effect at 10 minutes, rapid offset (minutes).
PHARMACEUTICS
- Formulations:
- Intravenous solution: 12.5 mg/mL, 1 mg/mL-D5%, 2 mg/mL-D5%, 4 mg/mL-D5%.
- Storage: Store at room temperature, do not freeze.
DOSE
- Adults and paediatrics:
- Initial: 0.5-1 mcg/kg/min IV infusion.
- Maintenance: 2-20 mcg/kg/min IV infusion.
- Maximum: 40 mcg/kg/min IV infusion.
INDICATIONS
- Short-term inotropic support in decompensated heart failure/ cardiogenic shock and after cardiac surgery
- Other uses:
- stress echocardiography
- Sepsis: added to norepinephrine in patients with sepsis-induced myocardial dysfunction or persistent hypoperfusion despite adequate fluid resuscitation and vasopressor therapy (Surviving Sepsis Campaign Guideline, 2021)
CONTRA-INDICATIONS
Absolute
- LVOTO
- Hypersensitivity
Relative
- Atrial fibrillation with rapid ventricular response; other tachycardias
- Hypertension
ADVERSE EFFECTS
- Cardiovascular:
- Tachycardia, arrhythmias, hypertension.
- Life-threatening: VT, VF, myocardial ischemia ((from increased O2 demand)
- Neurological:
- Headache, anxiety, tremor
- Gastrointestinal:
- Nausea, vomiting.
- Respiratory:
- dyspnoea.
- Metabolic:
- Hypoglycaemia, increased FFA concentration
- Immune:
- Increased NK cell activity
- Life-threatening: Allergic reactions (e.g., anaphylaxis)
- Other:
- Fever, leg cramps.
- Extravasation injury
- Tachyphylaxis (e.g. within 24-48h – due to GPCR kinase-mediated desensitization and downregulation of β-adrenergic receptors, especially in patients with chronic heart failure or prolonged catecholamine exposure)
DRUG-DRUG INTERACTIONS
- Monoamine Oxidase Inhibitors (MAOIs): Risk of hypertensive crisis due to enhanced catecholamine effects (e.g., phenelzine, tranylcypromine, selegiline, linezolid)
- Beta-blockers: May blunt dobutamine’s inotropic effects
- Nitrates (e.g., nitroprusside): Combined vasodilation may cause hypotension
PHARMACOKINETICS
- Absorption: 100% bioavailability via intravenous (IV) administration
- Distribution: Small volume of distribution (Vd) ≈ 0.2–0.3 L/kg
- Metabolism: Rapid hepatic and tissue metabolism via catechol-O-methyltransferase (COMT) to form 3-O-methyldobutamine, followed by glucuronidation. No significant metabolism via monoamine oxidase (MAO)
- Excretion: Primarily renal, as inactive metabolites; Half-life: ~2-3 minutes; Clearance 244 L/h
PREGNANCY AND LACTATION
- Pregnancy: Category B (no proven risk in humans).
- Lactation: Not recommended; effects on the nursing infant are unknown.
DOSE ADJUSTMENTS IN ORGAN FAILURES
- Renal Impairment: No specific dose adjustment required.
- Liver Impairment: No specific dose adjustment required.
- Renal Replacement Therapy: No specific dose adjustment required.
EVIDENCE
DOBERMANN-D (2024)
- Design: Randomised, double-blind, placebo-controlled trial; N = 100 (Dobutamine 50; Placebo 50)
- Intervention: Low-dose Dobutamine (5 μg/kg/min for 24h) vs Placebo post-PCI in AMI patients at risk of cardiogenic shock
- Primary Outcome: Peak plasma proBNP within 48 hours
- Results:
- Lower proBNP and improved hemodynamics in Dobutamine group
- Criticisms: Surrogate endpoint; small sample; single-center; short follow-up
- Conclusion: Early low-dose Dobutamine may reduce hemodynamic stress in high-risk AMI patients, but clinical outcome data are lacking.
DOREMI (Mathew et al, 2021)
- Design: Randomised, double-blind, single-center trial; N = 192 (Milrinone 96; Dobutamine 96)
- Intervention: Milrinone vs Dobutamine titrated for cardiogenic shock management
- Primary Outcome: Composite of in-hospital death, cardiac arrest, transplant, MI, stroke, or renal replacement therapy
- Results:
- Composite outcome: Milrinone 49% vs Dobutamine 54% (RR 0.90; p = 0.47)
- No significant differences in arrhythmias, ICU stay, or secondary outcomes
- Criticisms: Single-center limits generalizability; short follow-up; no long-term data
- Conclusion: Milrinone and dobutamine had similar efficacy and safety profiles in cardiogenic shock; choice may depend on patient-specific factors.
SURVIVE (Mebazaa et al, 2007)
- Design: Randomised, double-blind, multinational trial; N = 1,327 (Levosimendan 664; Dobutamine 663)
- Intervention: Levosimendan 24-hour IV infusion vs Dobutamine IV infusion up to 5 days
- Primary Outcome: All-cause mortality at 180 days
- Results:
- 180-day mortality: Levosimendan 26% vs Dobutamine 28% (HR 0.91; p = 0.40)
- Day 5 mortality: Levosimendan 3.4% vs Dobutamine 5.8% (HR 0.58; p = 0.05)
- BNP reduction significantly greater with Levosimendan (p < 0.001)
- Criticisms: No long-term survival benefit; post hoc subgroup findings; heterogeneity across sites
- Conclusion: Levosimendan showed early hemodynamic and biomarker benefits but no long-term mortality advantage over dobutamine.
CONTROVERSIES
- Lack of evidence: Evidence from clinical trials for the benefit of inotropes, and the choice of one inotrope over another, is generally lacking.
- Role of dobutamine after myocardial infarction, due to risk of increased myocardial oxygen demand.
- Role of dobutamine as an adjunctive agent (e.g. with noradrenaline and/or vasopressin) in septic shock.
PRACTICAL TIPS
- In clinical practice use of inotropes is guided by the clinical presentation, experience with inotropes at the clinical site, cost, and patient’s response to therapy.
- Monitoring: Continuous ECG, blood pressure, and urine output monitoring required.
- Administration: Use a calibrated electronic infusion device for accurate dosing. Preferably given via central route due to risk of extravasation injury (less than for vasoconstrictors like noradrenaline). Short-term use via peripheral IV access may be acceptable in emergencies.
- Pulmonary hypertension and right heart failure: milrinone is generally preferred to dobtuamine in these patients.
- Avoiding Errors: Ensure correct drug and dose to prevent confusion with dopamine.
- If co-adminstered with beta-blockers, dobutamine tends to have decreased chrontropic and inotropic effects, but TPR tends to increase (due to α1 agonism)
- “The case for dobutamine” (Reade, 2008):
- cheap
- titratable
- few metabolic adverse effects
- familiarity
- increases heart rate while causing vasodilation
- increases myocardial consumption but also increases coronary perfusion
- no lactic acidosis
TOXICOLOGY
- Risk Assessment: High doses can lead to severe hypertension, arrhythmias, and myocardial ischemia.
- Management: Discontinue infusion, supportive care, treat complications
- Consider phentolamine for extravasation injury.
REFERENCES
Journal articles
- Dubin A, Mugno M. The Effects of Dobutamine in Septic Shock: An Updated Narrative Review of Clinical and Experimental Studies. Medicina (Kaunas). 2024 Apr 30;60(5):751. doi: 10.3390/medicina60050751. PMID: 38792934; PMCID: PMC11123338.
- Mathew R, Di Santo P, Jung RG, Marbach JA, Hutson J, Simard T, Ramirez FD, Harnett DT, Merdad A, Almufleh A, Weng W, Abdel-Razek O, Fernando SM, Kyeremanteng K, Bernick J, Wells GA, Chan V, Froeschl M, Labinaz M, Le May MR, Russo JJ, Hibbert B. Milrinone as Compared with Dobutamine in the Treatment of Cardiogenic Shock. N Engl J Med. 2021 Aug 5;385(6):516-525. doi: 10.1056/NEJMoa2026845. PMID: 34347952.
- Mebazaa A, Nieminen MS, Packer M, Cohen-Solal A, Kleber FX, Pocock SJ, Thakkar R, Padley RJ, Põder P, Kivikko M; SURVIVE Investigators. Levosimendan vs dobutamine for patients with acute decompensated heart failure: the SURVIVE Randomized Trial. JAMA. 2007 May 2;297(17):1883-91. doi: 10.1001/jama.297.17.1883. PMID: 17473298.
- Nomoto Y, Jhonokosi H, Karasawa S. Natural killer cell activity and lymphocyte subpopulations during dobutamine infusion in man. Br J Anaesth. 1993 Aug;71(2):218-21. doi: 10.1093/bja/71.2.218. PMID: 8123395.
- Reade MC. The case for dobutamine. Crit Care Resusc. 2008 Sep;10(3):179. PMID: 18798712.
- Tuttle RR, Mills J. Dobutamine: development of a new catecholamine to selectively increase cardiac contractility. Circ Res. 1975 Jan;36(1):185-96. doi: 10.1161/01.res.36.1.185. PMID: 234805.
- Williams RS, Bishop T. Selectivity of dobutamine for adrenergic receptor subtypes: in vitro analysis by radioligand binding. J Clin Invest. 1981 Jun;67(6):1703-11. doi: 10.1172/jci110208. PMID: 6263950; PMCID: PMC370747.
Textbooks
- Brunton LL, Knollmann BC, eds. Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 14th ed. New York, NY: McGraw Hill; 2023.
- Scarth E, Smith S. Drugs in Anaesthesia and Intensive Care. 5th ed. Oxford, UK: Oxford University Press; 2016.
- Vanderah TW. Katzung’s Basic and Clinical Pharmacology. 16th ed. New York, NY: McGraw Hill; 2023.
FOAM and websites
- Deranged Physiology – Dobutamine
- The Bottom Line – DOREMI
References and Links
CCC Pharmacology Series
Respiratory: Bosentan, Delivery of B2 Agonists in Intubated Patients, Nitric Oxide, Oxygen, Prostacyclin, Sildenafil
Cardiovascular: Adenosine, Adrenaline (Epinephrine), Amiodarone, Classification of Vasoactive drugs, Clevidipine, Digoxin, Dobutamine, Dopamine, Levosimendan, Levosimendan vs Dobutamine, Milrinone, Noradrenaline, Phenylephrine, Sodium Nitroprusside (SNiP), Sotalol, Vasopressin
Neurological: Dexmedetomidine, Ketamine, Levetiracetam, Lignocaine, Lithium, Midazolam, Physostigmine, Propofol, Sodium Valproate, Sugammadex, Thiopentone
Endocrine: Desmopressin, Glucagon Therapy, Medications and Thyroid Function
Gastrointestinal: Octreotide, Omeprazole, Ranitidine, Sucralfate, Terlipressin
Genitourinary: Furosemide, Mannitol, Spironolactone
Haematological: Activated Protein C, Alteplase, Aprotinin, Aspirin, Clopidogrel, Dipyridamole, DOACs, Factor VIIa, Heparin, LMW Heparin, Protamine, Prothrombinex, Tenecteplase, Tirofiban, Tranexamic Acid (TXA), Warfarin
Antimicrobial: Antimicrobial Dosing and Kill Characteristics, Benzylpenicillin, Ceftriaxone, Ciprofloxacin, Co-trimoxazole / Bactrim, Fluconazole, Gentamicin, Imipenem, Linezolid, Meropenem, Piperacillin-Tazobactam, Rifampicin, Vancomycin
Analgesic: Alfentanil, Celecoxib, COX II Inhibitors, Ketamine, Lignocaine, Morphine, NSAIDs, Opioids, Paracetamol (Acetaminophen), Paracetamol in Critical Illness, Tramadol
Miscellaneous: Activated Charcoal, Adverse Drug Reactions, Alkali Therapies, Drug Absorption in Critical Illness, Drug Infusion Doses, Epidural Complications, Epidural vs Opioids in Rib Fractures, Magnesium, Methylene Blue, Pharmacology and Critical Illness, PK and Obesity, PK and ECMO, Sodium Bicarbonate Use, Statins in Critical Illness, Therapeutic Drug Monitoring, Weights in Pharmacology
Toxicology: Digibind, Flumazenil, Glucagon Therapy, Intralipid, N-Acetylcysteine, Naloxone, Propofol Infusion Syndrome
Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC