
![]()
Urea-Creatinine Ratio
OVERVIEW
Principle
- urea and creatinine both freely filtered at the glomerulus
- creatinine is not reabsorbed
- urea reabsorbed by tubules via regulation
- can be used as an indicator of the likely cause of renal failure
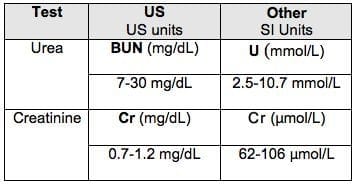
Normal Urea – 2.5-10.7mmol/L
Normal Creatinine – 62-106umol/L -> 0.062 – 0.106mmol/L (divide micromoles by 1000)
The relationship of urea and creatine is dependent on serum laboratory units used to determine the cause of acute kidney injury.
- In the US the urea is expressed as BUN (Blood Urea Nitrogen) in mg/dL.
- Elsewhere Urea (U) is expressed as mmol/L
- Similarly, Creatinine (Cr) is expressed as mg/dL in the US and µmol/L elsewhere
Conversion: SI to traditional units
- Plasma urea: 10 mmol/l = 27.8 mg/100 ml
- Plasma creatinine: 100 µmol/ – 1.13 mg/100 ml.
Therefore two ratio’s exist to compare serum Urea and Creatinine levels
- BUN : Cr ratio with US units of mg/dL : mg/dL – this is most commonly used in online calculators and converts the SI units to US units e.g. MDcalc
- Urea : Cr ratio with SI Units of mmol/L: mmol/L (providing Urea is >10mmol/L) – [note to calculate the Urea : Cr ratio it is required to convert the Creatinine from µmol/L to mmol/L] [hat tip Dr Julian Pecora]
- Cr : Urea ratio with SI Units of µmol/L: mmol/L (providing Urea is >10mmol/L)
CAUSES
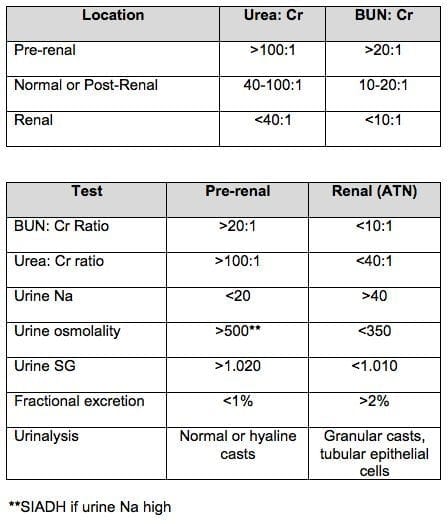
Urea:Creatinine Ratio (in the setting of renal failure / elevated creatinine)
- 40-100:1 – normal or post renal cause of AKI
- >100:1 – pre-renal cause (urea absorption increased compared to creatinine)
- <40:1 – intrinsic renal damage (urea unable to be absorbed -> become like creatinine -> ratio gets closer to 1)
Other causes:
INCREASED UREA:CREATININE RATIO – (Drivers Can use GPS)
- dehydration/prerenal failure
- corticosteroids
- GI haemorrhage
- protein-rich diet
- severe catabolic state
DECREASED UREA:CREATININE RATIO (I am a SIMPLE SR)
- severe liver dysfunction
- intrinsic renal damage
- malnutrition
- pregnancy
- low protein diet
- SIADH
- rhabdomyolysis
References
- Morgan DB, Carver ME, Payne RB. Plasma creatinine and urea: creatinine ratio in patients with raised plasma urea. Br Med J. 1977 Oct 8;2(6092):929-32
- Witting MD, Magder L, Heins AE, Mattu A, Granja CA, Baumgarten M. ED predictors of upper gastrointestinal tract bleeding in patients without hematemesis. Am J Emerg Med. 2006 May;24(3):280-5. PMID 16635697
- Urashima M, Toyoda S, Nakano T, Matsuda S, Kobayashi N, Kitajima H, Tokushige A, Horita H, Akatsuka J, Maekawa K. BUN/Cr ratio as an index of gastrointestinal bleeding mass in children. J Pediatr Gastroenterol Nutr1992 Jul;15(1):89-92. PMID 1403455.
- Feinfeld DA, Bargouthi H, Niaz Q, Carvounis CP. Massive and disproportionate elevation of blood urea nitrogen in acute azotemia. Int Urol Nephrol. 2002;34(1):143-5. PMID 12549657

Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC