
![]()
Bag-Valve-Mask (BVM) Ventilation
OVERVIEW
- Bag-Valve-Mask (BVM) apparatus are also known as manual resuscitators and as self-inflating resuscitation systems
- examples include LaerdalTM, AmbuTM, HsinerTM, MayoTM, and Air VivaTM
USES
- administration of high flow O2
- provision of PEEP (positive end-expiratory pressure)
- provision of controlled ventilation
- provision of augmentation of spontaneous ventilation
DESCRIPTION
- self-inflating resuscitation device
- bag made of plastic materials that re-expand after being manually collapsed
- various sizes e.g. Laerdal 240 mL, 500 mL, 1600 mL bag sizes for infants, children and adults
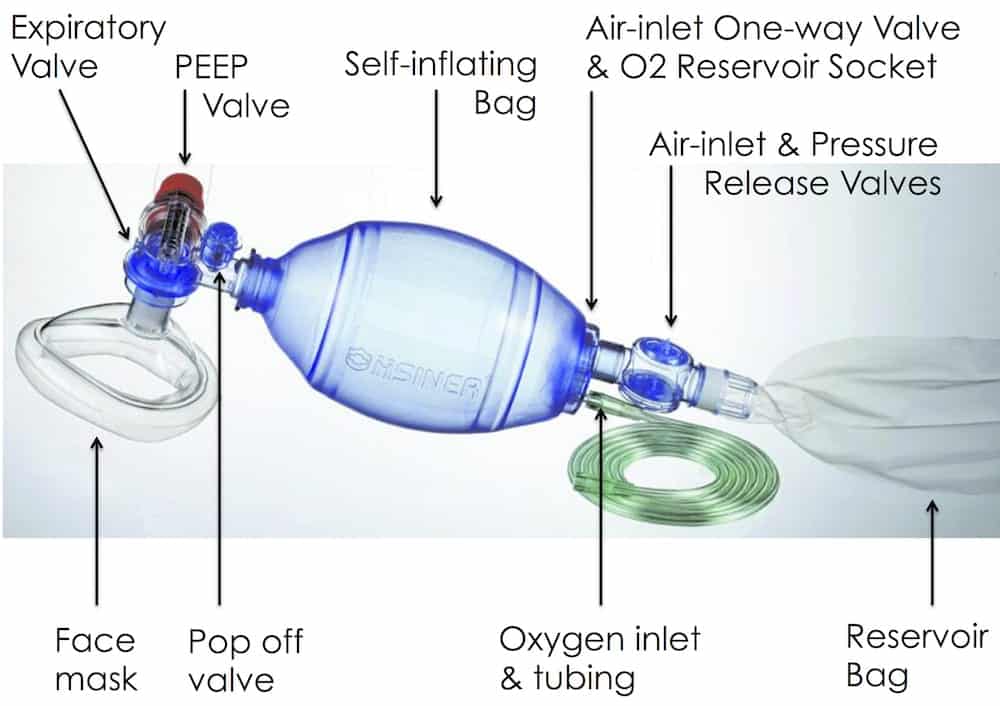
- oxygen inlet nipple
- air intake valve
- oxygen reservoir with two one way valves
- reservoir is at least the volume of the bag
- oxygen flow rate equal to, or higher than, the minute volume of the patient allows 100% oxygen to be delivered
- inlet valve allows room air to enter if fresh gas flow is inadequate and an outlet valve allow oxygen to flow out if pressure is excessive
- non-rebreathing valve that directs fresh flow of oxygen to the patient and prevents exhaled gas re-entering the bag
- standard 15 mm adapter for attaching to masks or tubes
- able to attach PEEP valve to exhalation port (either “built in” or detachable)
- can hold down pop off valve (releases at about 60 cmH2O) to give increased pressure in the circuit
- Masks come in a range of sizes and designs
- opaque or clear plastic
- firm or air inflated cushion
- mouldings vary but are designed to minimise dead space and fit
- some have specific names (e.g. Rendall Baker Mask for paediatrics)
METHOD OF INSERTION AND/OR USE
- High flow oxygen (e.g. 15 L/min) is attached to the system and it is attached to a mask or tube
- appropriate mask size
- place over mouth and nose
- tight fit
- open airway using two-handed thumbs down technique (with an assistant bagging) in preference to the less effective one-handed C-E grip to ensure airway patency (best if OPA and NPAs in situ too)
- the bag is used to deliver oxygen to a spontaneously breathing patient or the bag compressed to manually ventilate them via a mask or tube (an assistant can provide ventilations)
Remember JAWS for the two-handed two-thumbs down two person technique:
- Jaw thrust
- Airways (oral/nasal)
- Work together
- Slow, small squeeze — 6-7 cc/kg, over 1-2 seconds, at <12/min, using low pressure.
COMPLICATIONS
- easy to hyperventilate patients and limited ability to gauge tidal volumes
- unable to gauge lung compliance (cf. a ventilator or Water’s circuit)
- poor seal is common if one-handed CE grip is used
- gastric distension
- aspiration
- claustrophobia
- exhaled secretions and moisture can result in exhalation valve dysfunction and increased resistance to expiration
- risk of barotrauma if pop off valve close as unable to feel lung compliance with self-inflating bags
- if high free gas flows are not used high FiO2 will not be achieved
- equipment failure (e.g. due to incorrect assembly)
OTHER INFORMATION
Spontaneous ventilation
- Adminstered FiO2 during spontaneous ventilation can vary greatly between devices
- Laerdal: FiO2 0.96
- Hsiner: FiO2 0.75
- Mayo: FiO2 0.55
- sufficient negative inspiratory pressure is required to overcome the patient inspiratory valve, otherwise, air will be entrained instead of oxygen
- some duckbill valves are difficult to overcome when spontaneously breathing
- patients with reduced respiratory effort are particularly at risk
- As a safeguard in spontaneously breathing patients it is useful to coordinate ‘assist’ positive pressure ventilation with the patient’s spontaneous efforts to ensure that the patient inspiratory valve is opening
Edentulous patients
- If the patient is edentulous, then adjust the position of the mask like so:

Fom Racine SX, et al (2010), image from EM Updates (click image for source)
Alternatives to BVM
- use a ventilator to provide non-invasive ventilation
- use of a Mapleson C (Waters circuit)
- in paediatrics, use of Mapleson E (Jackson-Ress modification of the Ayre’s T-pieces)
VIDEOS
References and Links
Introduction to ICU Series
Introduction to ICU Series Landing Page
DAY TO DAY ICU: FASTHUG, ICU Ward Round, Clinical Examination, Communication in a Crisis, Documenting the ward round in ICU, Human Factors
AIRWAY: Bag Valve Mask Ventilation, Oropharyngeal Airway, Nasopharyngeal Airway, Endotracheal Tube (ETT), Tracheostomy Tubes
BREATHING: Positive End Expiratory Pressure (PEEP), High Flow Nasal Prongs (HFNP), Intubation and Mechanical Ventilation, Mechanical Ventilation Overview, Non-invasive Ventilation (NIV)
CIRCULATION: Arrhythmias, Atrial Fibrillation, ICU after Cardiac Surgery, Pacing Modes, ECMO, Shock
CNS: Brain Death, Delirium in the ICU, Examination of the Unconscious Patient, External-ventricular Drain (EVD), Sedation in the ICU
GASTROINTESTINAL: Enteral Nutrition vs Parenteral Nutrition, Intolerance to EN, Prokinetics, Stress Ulcer Prophylaxis (SUP), Ileus
GENITOURINARY: Acute Kidney Injury (AKI), CRRT Indications
HAEMATOLOGICAL: Anaemia, Blood Products, Massive Transfusion Protocol (MTP)
INFECTIOUS DISEASE: Antimicrobial Stewardship, Antimicrobial Quick Reference, Central Line Associated Bacterial Infection (CLABSI), Handwashing in ICU, Neutropenic Sepsis, Nosocomial Infections, Sepsis Overview
SPECIAL GROUPS IN ICU: Early Management of the Critically Ill Child, Paediatric Formulas, Paediatric Vital Signs, Pregnancy and ICU, Obesity, Elderly
FLUIDS AND ELECTROLYTES: Albumin vs 0.9% Saline, Assessing Fluid Status, Electrolyte Abnormalities, Hypertonic Saline
PHARMACOLOGY: Drug Infusion Doses, Summary of Vasopressors, Prokinetics, Steroid Conversion, GI Drug Absorption in Critical Illness
PROCEDURES: Arterial line, CVC, Intercostal Catheter (ICC), Intraosseous Needle, Underwater seal drain, Naso- and Orogastric Tubes (NGT/OGT), Rapid Infusion Catheter (RIC)
INVESTIGATIONS: ABG Interpretation, Echo in ICU, CXR in ICU, Routine daily CXR, FBC, TEG/ROTEM, US in Critical Care
ICU MONITORING: NIBP vs Arterial line, Arterial Line Pressure Transduction, Cardiac Output, Central Venous Pressure (CVP), CO2 / Capnography, Pulmonary Artery Catheter (PAC / Swan-Ganz), Pulse Oximeter
Journal articles
- El-Orbany M, Woehlck HJ. Difficult mask ventilation. Anesth Analg. 2009 Dec;109(6):1870-80. PMID: 19923516
- Gerstein NS, Carey MC, Braude DA, Tawil I, Petersen TR, Deriy L, Anderson MS. Efficacy of facemask ventilation techniques in novice providers. J Clin Anesth. 2013 May;25(3):193-7. PMID: 23523573.
- Hart D, Reardon R, Ward C, Miner J. Face mask ventilation: a comparison of three techniques. J Emerg Med. 2013 May;44(5):1028-33. PMID: 23473817.
- Joffe AM, Hetzel S, Liew EC. A two-handed jaw-thrust technique is superior to the one-handed “EC-clamp” technique for mask ventilation in the apneic unconscious person. Anesthesiology. 2010 Oct;113(4):873-9. PMID: 20808210.
- Khoury A, Hugonnot S, Cossus J, et al. From mouth-to-mouth to bag-valve-mask ventilation: evolution and characteristics of actual devices – a review of the literature. Biomed Res Int. 2014;2014:762053. [article]
- Racine SX, et al (2010). Face mask ventilation in edentulous patients: a comparison of mandibular groove and lower lip placement. Anesthesiology, 112 (5), 1190-3 PMID: 20395823
FOAM and web resources
- AirwayCam — Face Mask Ventilation
- EMCRIT — Wee – What the heck is a Mapleson B Circuit and Why You Probably Shouldn’t Care (2014)
- Resus.ME — Thenar Eminence Based Medicine

Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC

[…] Nickson, C. (2019, April 22). Bag-Valve-Mask (BVM) Ventilation. Retrieved from Life in the fastlane: https://litfl.com/bag-valve-mask-bvm-ventilation/ […]