
![]()
Underwater Seal Chest Drainage System
OVERVIEW
A system that allows drainage of the pleural space using an airtight system to maintain subatmospheric intrapleural pressure; the underwater seal acts a one-way valve
USES
- drainage of pleural air, blood or other fluid to allow re-expansion of lung
DESCRIPTION
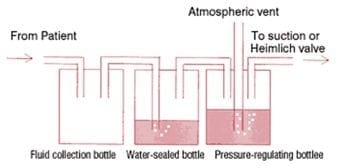
3 bottle system
1 bottle system
- essentially the water-sealed bottle of the 3 bottle system directly attached to the intercostal catheter, with a second tube open to air
METHOD OF USE
3-bottle system
- a trap or collection bottle is interposed between the intercostal catheter and the underwater-seal bottle and a third bottle, called the manometer or pressure-regulating bottle, is added after the underwater-seal bottle
- modern drains incorporate three separate bottles into one unit
- bottle A = fluid trap or collection bottle, can be independently emptied and allows accurate record of drainage amount
- bottle B = underwater seal drain, maintained at a predetermined level whilst still allowing for drainage of pleural fluid (if bubbling continuously -> bronchopleural fistula)
- bottle C = manometer or pressure-regulating bottle allows suction to be attached and should bubble continuously
- The maximum negative pressure (in cm H2O) generated by suction equals to the distance (in cm) the vent tube is below the water line (this can be adjusted)
- The negative pressure generated by the vent tube is independent of the amount of pleural drainage that is collected in the trap bottle
1-bottle system
- chest drain is connected by collecting tubing to a tube approximately 3 cm under water (the seal) in the underwater-seal bottle
- another vent tube is open to atmosphere
- pleural pressure greater than +3 cm water will force air or fluid from the pleural space into the bottle while negative pressure in the pleural space will suck fluid up the tube
- As long as the underwater-seal bottle is well below the patient (e.g., on the floor beside the patient), the hydrostatic pressure of the fluid column in the tube will counterbalance the negative pleural pressure and prevent water from being sucked into the pleural space
- The hydrostatic pressure is proportional to the height of the fluid column
- A disadvantage of this single bottle system is that, as liquid content (blood, pus, effusion fluid) is expelled from the pleural space and collects in the underwater-seal bottle, the seal tube becomes immersed deeper under water and the pressure required to force more contents into the bottle increases thus impeding the clearance of the pleural collection
OTHER INFORMATION
Safety features
- first tube connecting drain to drainage bottles must be wide to decreased resistance
- volume capacity of this tube should exceed ½ of patient’s maximum inspiratory volume (otherwise H2O may enter chest)
- volume of H2O in bottle B should exceed ½ patient’s maximum inspiratory volume to prevent indrawing of air during inspiration
- drain should always stay at least 45cm below patient (prevention of removed fluid or H2O refluxing into patient)
- clamp drain when moving
- H2O level above tube in the manometer bottle determines the amount of suction applied before air drain through tube (safety suction limiting device)
- if suction is turned off then tubing must be unplugged -> so air can escape into atmosphere (otherwise a tension pneumothorax)
- should not be applied following pneumonectomy
Complications
- Kinking
- occlusion
- retrograde flow of fluid may occur if the collection chamber is raised above the level of the patient
- clamping may cause a tension pneumothorax
- the drains must be maintained upright to maintain the seal
- glass bottles can break
Heimlich valves
- unidirectional flutter valve used to replace underwater seal drains (e.g. when being transported)
- consists of a tubing assembly and sealed transparent housing with tubing connection ends to attach to the chest drain and a collection bag
References and Links
Introduction to ICU Series
Introduction to ICU Series Landing Page
DAY TO DAY ICU: FASTHUG, ICU Ward Round, Clinical Examination, Communication in a Crisis, Documenting the ward round in ICU, Human Factors
AIRWAY: Bag Valve Mask Ventilation, Oropharyngeal Airway, Nasopharyngeal Airway, Endotracheal Tube (ETT), Tracheostomy Tubes
BREATHING: Positive End Expiratory Pressure (PEEP), High Flow Nasal Prongs (HFNP), Intubation and Mechanical Ventilation, Mechanical Ventilation Overview, Non-invasive Ventilation (NIV)
CIRCULATION: Arrhythmias, Atrial Fibrillation, ICU after Cardiac Surgery, Pacing Modes, ECMO, Shock
CNS: Brain Death, Delirium in the ICU, Examination of the Unconscious Patient, External-ventricular Drain (EVD), Sedation in the ICU
GASTROINTESTINAL: Enteral Nutrition vs Parenteral Nutrition, Intolerance to EN, Prokinetics, Stress Ulcer Prophylaxis (SUP), Ileus
GENITOURINARY: Acute Kidney Injury (AKI), CRRT Indications
HAEMATOLOGICAL: Anaemia, Blood Products, Massive Transfusion Protocol (MTP)
INFECTIOUS DISEASE: Antimicrobial Stewardship, Antimicrobial Quick Reference, Central Line Associated Bacterial Infection (CLABSI), Handwashing in ICU, Neutropenic Sepsis, Nosocomial Infections, Sepsis Overview
SPECIAL GROUPS IN ICU: Early Management of the Critically Ill Child, Paediatric Formulas, Paediatric Vital Signs, Pregnancy and ICU, Obesity, Elderly
FLUIDS AND ELECTROLYTES: Albumin vs 0.9% Saline, Assessing Fluid Status, Electrolyte Abnormalities, Hypertonic Saline
PHARMACOLOGY: Drug Infusion Doses, Summary of Vasopressors, Prokinetics, Steroid Conversion, GI Drug Absorption in Critical Illness
PROCEDURES: Arterial line, CVC, Intercostal Catheter (ICC), Intraosseous Needle, Underwater seal drain, Naso- and Orogastric Tubes (NGT/OGT), Rapid Infusion Catheter (RIC)
INVESTIGATIONS: ABG Interpretation, Echo in ICU, CXR in ICU, Routine daily CXR, FBC, TEG/ROTEM, US in Critical Care
ICU MONITORING: NIBP vs Arterial line, Arterial Line Pressure Transduction, Cardiac Output, Central Venous Pressure (CVP), CO2 / Capnography, Pulmonary Artery Catheter (PAC / Swan-Ganz), Pulse Oximeter

Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC