
![]()
Human Factors
OVERVIEW
- Human failures rather than technical failures are the greatest threat to complex and potentially hazardous systems such as healthcare systems.
- In aviation, over 70% of adverse events are due to human factors – data suggests a similar rate in healthcare
- Managing the human risks will never be 100% effective. Human fallibility can be moderated, but it cannot be eliminated.
ERROR
Different types of error:
- have different underlying mechanisms
- occur in different parts of the organization
- require different methods of risk management
Error types
- Execution failures (actions deviate from the intention)
— Slips (attention failures), lapses (memory failures), trips, and fumbles - Planning or problem solving failures (things go to plan, but the plan is wrong)
— mistakes
Mistakes
- Rule-based mistakes
— misapplication of a good rule
— application of a bad rule
— non-application of a good rule - Knowledge-based mistakes
— a novel problem where the solution has to be worked out
— slow resource-intensive reasoning based on an incomplete or inaccurate ‘mental model’ that is subject to cognitive biases
VIOLATIONS
- Violations are deviations from safe operating practices, procedures, standards, or rules.
- may be deliberate or unintentional
- deliberate violations are distinct from errors as they involve motivational problems, not problems with information handling
- violations involve social context, errors do not
- motivational and organizational remedies are needed rather than improved information quality and delivery
3 main groups
- routine violations (cutting corners whenever possible)
- optimizing violations (actions taken for personal rather than task-orientated reasons)
- necessary or situational violations (needed to get the task done because the rules or procedures are seen as inappropriate to the task)
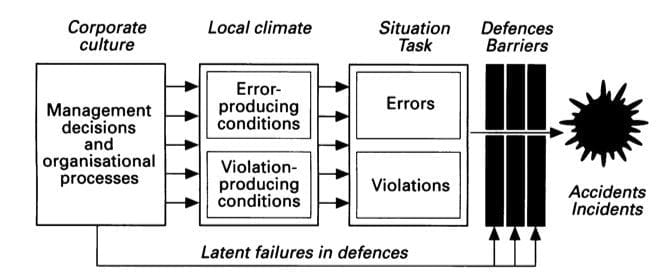
HUMAN FAILURES
Two types
- active
- latent
Active failures
- unsafe acts (errors or violations) committed by those in direct contact with the patient (at “the sharp end”)
- almost immediate effect
Latent failures
- Latent failures arise in organizational and managerial spheres
- adverse effects may take a long time to become evident
- become evident when combined with a local triggering event
PRINCIPLED RISK MANAGEMENT
Retro-fixes to prevent events, sanctions, retraining and other ‘anti-personnel’ countermeasures are ineffective
- those at the sharp end are the inheritors of the accident sequence, they do not choose to error and are not necessarily especially prone to error – if the individual cannot control it, neither can the organisation
- psychological factors are the last links in the chain and the least manageable
- accidents are rarely due to single unsafe acts, as long as the alternate errors remain the potential for other acts to lead to adverse events remains
- these countermeasures create a false sense of security
- increased automation does not prevent human factors from leading to adverse events, just changes their nature (as systems are made more opaque, errors often become less likely, but with greater potential for mistakes)
EFFECTIVE RISK MANAGEMENT
Effective risk managements aims to improve human performance at all levels of the system, rather than to minimise particular errors and mistakes.
- Effective risk management depends critically on a confidential and preferable anonymous incident monitoring system that records the individual, task, situational, and organisational factors associated with incidents and near misses.
- Effective risk management means the simultaneous and targeted deployment of limited remedial resources at different levels of the system: the individual or team, the task, the situation, and the organisation as a whole.
- Automation and increasing advanced equipment do not cure human factors problems, they merely relocate them. In contrast, training people to work effectively in teams costs little, but has achieved significant enhancements of human performance in aviation.
- People do not act in isolation. Their behaviour is shaped by circumstances. The same is true for errors and violations. The likelihood of an unsafe act being committed is heavily influenced by the nature of the task and by the local workplace conditions. These, in turn, are the product of “upstream” organizational factors. Great gains in safety can ve achieved through relatively small modifications of equipment and workplaces.
Effective risk management addresses:
- team factors
- task factors
- situational factors
- organizational factors
TEAM FACTORS
Important team factors that reduce error identified from aviation disasters applied to medical teams:
- establishment of team concept and environment for open communications
- briefings are thorough and address team coordination and planning for all important contingencies
- all relevant participants are included as part of the team
- group climate is appropriate to the operational situation (social interaction must not interfere with necessary tasks)
- team members ask questions regarding team actions
- team members speak up and persist until there is appropriate resolution
- team leader coordinates team activities, establishes proper balance between authority and team participation, and is decisvie when required
- workload and task distribution is clearly communicated and acknowledged by team members and appropriate time is allocated to tasks
- secondary tasks are appropriately prioritized so that sufficient resources are allocated to complete primary tasks
- team prepares of expected contingencies
- when conflicts arise team remains focused on the problem at hand
- team members listen actively to opinions and ideas and admit when they are wrong
TASK FACTORS
- identify and modify tasks and task elements that are prone to failure
- efficient incident monitoring
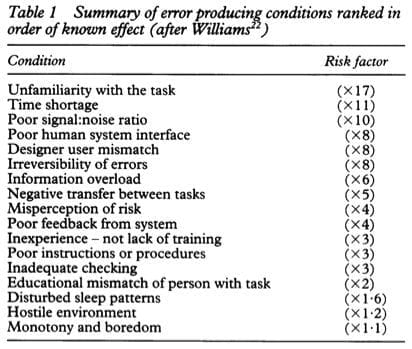
SITUATIONAL FACTORS
7 broad categories of error producing conditions:
- high workload
- inadequate knowledge, ability or experience
- poor interface design
- inadequate supervision or instruction
- stressful environment
- mental state (fatigue, boredom, etc)
- change
7 broad categories of violation producing conditions:
- lack of safety culture
- lack of concern
- poor morale
- norms condoning violation
- “can do” attitudes
- apparently meaningless or ambiguous rules
ORGANIZATIONAL FACTORS
- accident and incident reporting procedures should record events that occur at all levels, and ideally be confidential and anonymous
- continuous sampling of measures of quality are also important determinants of patient safety, however the parameters to assess may be arbitrary
- simultaneous and targeted deployment of limited remedial resources at different levels of the system
References and Links
Introduction to ICU Series
Introduction to ICU Series Landing Page
DAY TO DAY ICU: FASTHUG, ICU Ward Round, Clinical Examination, Communication in a Crisis, Documenting the ward round in ICU, Human Factors
AIRWAY: Bag Valve Mask Ventilation, Oropharyngeal Airway, Nasopharyngeal Airway, Endotracheal Tube (ETT), Tracheostomy Tubes
BREATHING: Positive End Expiratory Pressure (PEEP), High Flow Nasal Prongs (HFNP), Intubation and Mechanical Ventilation, Mechanical Ventilation Overview, Non-invasive Ventilation (NIV)
CIRCULATION: Arrhythmias, Atrial Fibrillation, ICU after Cardiac Surgery, Pacing Modes, ECMO, Shock
CNS: Brain Death, Delirium in the ICU, Examination of the Unconscious Patient, External-ventricular Drain (EVD), Sedation in the ICU
GASTROINTESTINAL: Enteral Nutrition vs Parenteral Nutrition, Intolerance to EN, Prokinetics, Stress Ulcer Prophylaxis (SUP), Ileus
GENITOURINARY: Acute Kidney Injury (AKI), CRRT Indications
HAEMATOLOGICAL: Anaemia, Blood Products, Massive Transfusion Protocol (MTP)
INFECTIOUS DISEASE: Antimicrobial Stewardship, Antimicrobial Quick Reference, Central Line Associated Bacterial Infection (CLABSI), Handwashing in ICU, Neutropenic Sepsis, Nosocomial Infections, Sepsis Overview
SPECIAL GROUPS IN ICU: Early Management of the Critically Ill Child, Paediatric Formulas, Paediatric Vital Signs, Pregnancy and ICU, Obesity, Elderly
FLUIDS AND ELECTROLYTES: Albumin vs 0.9% Saline, Assessing Fluid Status, Electrolyte Abnormalities, Hypertonic Saline
PHARMACOLOGY: Drug Infusion Doses, Summary of Vasopressors, Prokinetics, Steroid Conversion, GI Drug Absorption in Critical Illness
PROCEDURES: Arterial line, CVC, Intercostal Catheter (ICC), Intraosseous Needle, Underwater seal drain, Naso- and Orogastric Tubes (NGT/OGT), Rapid Infusion Catheter (RIC)
INVESTIGATIONS: ABG Interpretation, Echo in ICU, CXR in ICU, Routine daily CXR, FBC, TEG/ROTEM, US in Critical Care
ICU MONITORING: NIBP vs Arterial line, Arterial Line Pressure Transduction, Cardiac Output, Central Venous Pressure (CVP), CO2 / Capnography, Pulmonary Artery Catheter (PAC / Swan-Ganz), Pulse Oximeter
- Understanding adverse events: human factors. Qual Health Care. 1995 Jun;4(2):80-9. PMC1055294.

Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC