
![]()
Eponymous Fractures
Eponymous fractures, fracture-dislocations and classifications systems are often named after the physician who first described them, or popularised the naming convention or operative repair.
Eponymous Orthopedic Injuries
[hide]
- Bankart Lesion (1923)
- Bosworth fracture (1947)
- Cedell fracture (1974)
- Chopart amputation (1792)
- Cotton fracture (1915)
- Danis-Weber classification (1949, 1972)
- Freiberg infraction (1914)
- Gosselin fracture (1855)
- Hawkins classification (1970)
- Jones Fracture (1902)
- Köhler disease I (1908)
- Lauge-Hansen classification of ankle injury (1950)
- Lisfranc joint (1815)
- Maisonneuve Fracture (1840)
- Pellegrini-Stieda syndrome (1905/1908)
- Pott fracture (1768)
- Segond fracture (1879)
- Shepherd fracture (1882)
- Tillaux-Chaput fracture (1876, 1907)
- Wagstaffe-Le Fort Fracture (1875, 1886)
Bankart Lesion (1923)

Bankart lesion Fracture of the antero-inferior glenoid rim with detachment of the glenoid labrum. Associated with anterior shoulder dislocations.
- Arthur Sidney Blundell Bankart (1879- 1951) British orthopaedic surgeon.
- Bankart ASB. Recurrent or habitual dislocation of the shoulder joint. Br Med J. 1923 Dec 15; 2(3285): 1132–1133.
Bosworth fracture (1947)

Bosworth fracture-dislocation is an archaic eponym for rare ankle injury in which the proximal fibular fragment is entrapped (fixed displacement) behind the tibia, frequently irreducible by closed methods. Archaic term for ankle fracture-dislocation
- David Marsh Bosworth (1897 – 1979) American orthopedic surgeon.
- Bosworth DM. Fracture-dislocation of the ankle with fixed displacement of the fibula behind the tibia. J Bone Joint Surg Am. 1947; 29(1): 130-5.
Cedell fracture (1974)

Cedell fracture is a posterior talar process fracture with injury to the posteromedial tubercle caused by forced dorsiflexion and pronation.
Fracture of the posterior process of the talus is an uncommon injury that is often missed on plain X-Ray and misdiagnosed as ankle sprain. In one case series, 17 of 20 patients with fractures were misdiagnosed as an ankle sprain.
- Carl-Axel Cedell (1932 – ) Swedish orthopaedic surgeon
- Cedell CA. Rupture of the posterior talotibial ligament with the avulsion of a bone fragment from the talus. Acta Orthop Scand. 1974; 45(3): 454-461
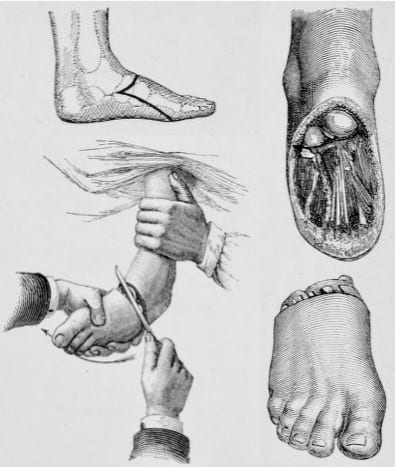
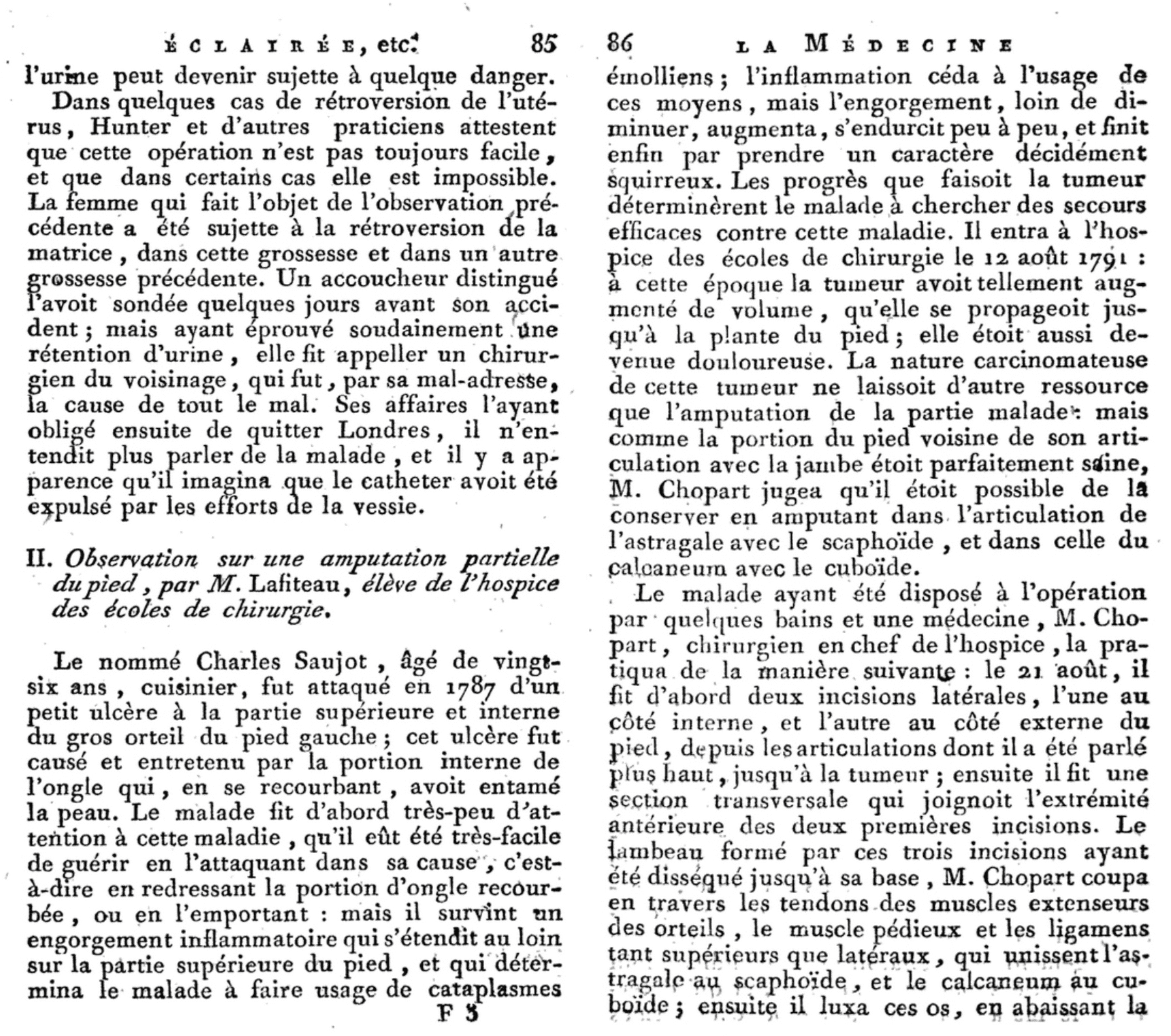
Chopart amputation (1792)

The mid-tarsal joint is also known as the Chopart joint. Chopart disarticulated this joint when performing forefoot amputations (Chopart amputation). A Chopart fracture-dislocation involves a midtarsal joint (talonavicular and calcaneocuboid) dislocation with associated fractures.
Chopart’s student, Lafiteau provided the first description of Chopart’s method of partial amputation of the foot and Chopart’s joint in Volume IV of Fourcroy ‘La médecine éclairée par les sciences physiques‘ in 1792. The fracture-dislocation was attributed at a later date.
- François Chopart (1743 – 1795) was a French Surgeon.
- Lafiteau. ‘Observation sur une amputation partielle du pied.’ In: Antoine François Fourcroy. La médecine éclairée par les sciences physiques, ou Journal des découvertes relatives aux différentes parties de l’art de guéri. Paris, chez Buisoon, 1792 [Volume IV: 85-86; 87-88].
Chopart amputation Garrè, 1922
Cotton fracture (1915)

Cotton fracture is a fracture of the ankle involving the lateral malleolus, medial malleolus and distal posterior aspect of the tibia (posterior malleolus). [aka *trimalleolar fracture ]
- Frederic Jay Cotton (1869 – 1939) was an American orthopedic surgeon.
- Cotton FJ. A new type of ankle fracture. JAMA. 1915; 64: 318–321.
Danis-Weber classification (1949, 1972)

The Danis-Weber classification (more commonly – the Weber classification) is a simple method of describing ankle fractures.
It has three categories (Type A, B and C.) based primarily upon the fracture of the fibula. The higher (more proximal) the fibular fracture, the greater the likelihood for ankle mortise insufficiency. first described by Robert Danis in 1949 and later modified and popularised by Bernhard Georg Weber in 1972, 10 years after Danis’ death.
- Robert Danis (1880 – 1962) Belgian general surgeon.
- Danis R. Les fractures malleolaires. In: Danis R. Theorie et pratique de l’osteosynthese. Masson et Cie, Paris, 1949.
- Bernhard Georg Weber (1927 – 2002) Swiss surgeon.
- Weber BG. Die Verletzungen des oberen Sprunggelenkes (The injuries of the upper ankle). Huber 1972 (2e)
Freiberg infraction (1914)

Osteochondrosis of the metatarsal heads (typically the 2nd metatarsal head) characterized pathologically by subchondral bone collapse, osteonecrosis, and cartilaginous fissures. Freiberg infraction is more common in women and most commonly manifests during adolescence (aged 10-18 years). Bilateral presentation in 10% of cases. Cause unknown and probably multi-factorial. High-heeled shoes have been implicated as a causative factor.
In 1913, Freiberg presented a paper to the Southern Surgical and Gynecological Association. He reported the cases of six young women presenting with a painful limp and discomfort localized to the second metatarsal, the first patient presenting in 1903. Freiberg employed used the term ‘infraction’ as the diagnosis (archaic term for fracture without displacement implying trauma as the cause).
Köhler called out Freiberg for an ‘incomplete‘ description of ‘metatarsal infraction‘ lacking mention of the widening of the joint line; thickening of the shaft of the metatarsal and obliteration of the neck. Process often referred to as Köhler disease II
- Albert Henry Freiberg (1868 – 1940) was an American Orthopedic Surgeon.
- Freiberg AH. Infraction of the second metatarsal – a typical injury. Transactions of the Southern Surgical and Gynecological Association 1914; 26: 171-174.
Gosselin fracture (1855)

Gosselin fracture is a V-shaped fracture of the distal tibia with extension into the tibial plafond, dividing it into anterior and posterior segments
- Léon Athanase Gosselin (1815 – 1887) was a French Surgeon.
- Gosselin LA. Les fractures en V du tibia. Bulletins et mémoires de la Société de chirurgie de Paris. 1855 p262
Hawkins classification (1970)

Classification system for talar neck fractures. Hawkins originally described Types I-III in 1970 with Canale and Kelly adding Type IV in 1978
- Leland Greene Hawkins (1933 – 1991) American orthopedic surgeon
- Hawkins LG. Fractures of the neck of the talus. J Bone Joint Surg Am. 1970; 52(5): 991-1002
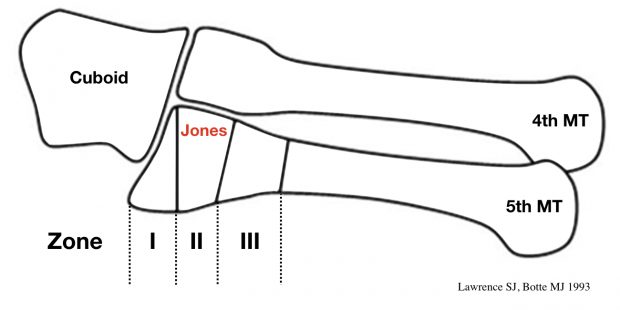
Jones Fracture (1902)

Fracture of the proximal diaphysis of the 5th metatarsal, distal to the tuberosity, without joint involvement. Caused by foot inversion / twisting and repetitive stress. First described by Robert Jones on himself after he injured his foot dancing. In 1902 he wrote up a case report of five similar injuries specifically noting that the fracture is caused by ‘indirect violence’
Whilst dancing, I trod on the outer side of my foot, my heel at the moment being off the ground. Something gave way midway down my foot, and I at once suspected a rupture of the peroneus longus tendon…I hobbled down-stairs to my colleague…to X-ray my foot. This was done, and the fifth metatarsal was found fractured about three-fourths of an inch from its base.
Jones R, Ann Surg. 1902: 697
- Sir Robert Jones (1857-1933) was a Welsh General and Orthopaedic Surgeon and part time Roentgenologist.
- Jones R. Fracture of the Base of the Fifth Metatarsal Bone by Indirect Violence. Ann Surg. 1902;35(6):697–700
Jones fracture and current classification

Köhler disease I (1908)

Köhler disease is a rare, self-limiting, avascular necrosis (osteonecrosis) of the navicular bone in children. Adult onset osteonecrosis of the tarsal navicular is known as Müller-Weiss syndrome (MWS) (also Brailsford disease)
- Alban Köhler (1874 – 1947) was a German Radiologist
- Köhler A. Uber eine häufige, bisher anscheinend unbekannte Erkrankung einzelner kindlicher Knochen. Munchener medizinische Wochenschrift, 1908; 55: 1923-5
- Walther Müller (1888 – 1949); Konrad Weiss (1891 – 1976); James F Brailsford (1888 – 1961)
- Müller W. Über eine eigenartige doppelseitige Veränderung des Os naviculare pedis beim Erwachsenen. Deutsche Zeitschrift für Chirurgie, Leipzig, 1927; 201: 84-87.
- Weiss K. Über die “Malazie” des Os naviculare pedis. RöFo: Fortschritte auf dem Gebiete der Röntgenstrahlen, 1927; 45: 63-67.
- Brailsford JF. Osteochondritis of the adult tarsal navicular. J Bone Joint Surg Am 1939; 21: 111-120
Lauge-Hansen classification of ankle injury (1950)
The Lauge-Hansen classification of ankle injuries was developed on the basis of predictable fracture patterns defined by injury mechanism and resultant radiological findings in 1950.
The Lauge-Hansen classification requires three radiographic views of the ankle (anteroposterior, mortise and lateral) and is characterised with specific two-word descriptors of the injury mechanism: The First word: describes the position of the foot at the time of injury (supination or pronation) and the Second word: describes the deforming force direction (abduction, adduction, or external rotation)
- Niels Lauge-Hansen (1899 – 1976) Danish Radiologist.
- Lauge-Hansen N. Fractures of the ankle. II. Combined experimental-surgical and experimental-roentgenologic investigations. Arch Surg. 1950; 60(5): 957-85.
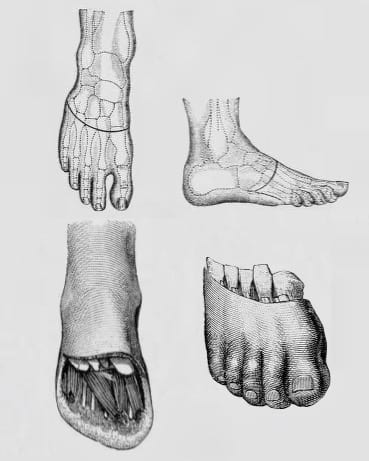
Lisfranc joint (1815)

Lisfranc is eponymously associated with his tarsometatarsal forefoot amputation (Lisfranc amputation). However, Lisfranc was not the first to describe the procedure, with William Hey (1736-1819) first performing and recording the procedure in 1803.
In 1815, Lisfranc described and refined the disarticulation of the forefoot at the tarsometatarsal joint complex which joins the forefoot and midfoot (Lisfranc joint). He defined the coup de maître of his disarticulation being the incision of the interosseous ligament (subsequently referred to as the Lisfranc ligament)
Lisfranc’s description of amputation through the tarsal-metatarsal joints requires several pages to describe it, but it took only 1 minute for him to perform it — not too short a time for the unanesthetized patient
Cassebaum WH, 1963
Note: the Lisfranc ligament complex includes the dorsal, interosseous, and plantar ligaments which connect C1 (medial cuneiform) to M2 (2nd metatarsal base).
Lisfranc injury refers to disruption of the tarsometatarsal joint. Injuries range from sprain (minor diastasis) through to tarsometatarsal fracture-dislocation.
- Jacques Lisfranc de St. Martin (1787 – 1847) was a French Surgeon.
- Hey W. Excision of the metatarsal bones. In: Practical observations in surgery. 1803: 530-537
- Lisfranc J. Nouvelle méthode opératoire pour l’amputation partielle du pied de son articulation tarsométatarsienne. methode precedee des nombreuses modifications qu’a subies celle de Chopart. 1815
Lisfranc amputation Garrè, 1922
{kind=link}
{kind=link}
Maisonneuve Fracture (1840)

Maisonneuve fracture is a spiral fracture of the upper third of the fibula associated with a tear of the distal tibiofibular syndesmosis and the interosseous membrane.
There is an associated fracture of the medial malleolus or rupture of the deep deltoid ligament. Rupture of the stabilizing ligaments of the distal tibiofibular syndesmosis will result in widening of the ankle mortise on radiographs. Additional findings such as avulsion fracture of the medial or posterior malleoli, or tear of the deltoid ligaments may also be present
- Jacques Gilles Maisonneuve (1809 – 1897) French Surgeon.
- Maisonneuve JG. Recherches sur la fracture du péroné. Archives générales de médecine 1840; 7 :165-187 and 433-473
Pellegrini-Stieda syndrome (1905/1908)

Köhler-Pellegrini-Stieda lesion: Ossification in or near the tibial collateral ligament (medial femoral collateral ligament) adjacent to the margin of the medial femoral condyle. Ossified post-traumatic lesion (presumed secondary to Stieda fracture)
- Alban Köhler (1874 – 1947) was a German Radiologist.
- Köhler A. Die normale und pathologische Anatomie des Hüftgelenks und Oberschenkels in röntgenographischer Darstellung. Hamburg, Lucas Gräfe & Sillem, 1905
- Augusto Pellegrini (1877 – 1958) was an Italian Surgeon.
- Pellegrini A. Ossificazione traumatica del ligamento collaterale tibiale dell’articolazione del ginocchio sinistro. [Traumatic calcification of the collateral tibial ligament of the knee joint] Clinica moderna (Firenze) 1905; 11: 433-439
- Eugen Julius Karl Paul Alfred Stieda (1869 – 1945) was a German Surgeon.
- Stieda A. Uber eine typische verletzung am unteren femurende. Archiv für Klinische Chirurgie, 1908; 85: 815-826
Pott fracture (1768)

Pott fracture is an archaic eponym for fracture of the distal fibula, 2–3 inches proximal to the ankle joint. Effectively a fracture-dislocation of the ankle, involving a fracture of the fibula, disruption of the deltoid ligaments with an intact tibiofibular ligament resulting in lateral displacement of the talus.
- Sir Percivall Pott (1714 – 1788) English surgeon.
- Pott P. Some few general remarks on fractures and dislocations. 1768: 217-260
Segond fracture (1879)

Segond fracture: Avulsion fracture (small) of the lateral surface of the lateral tibial condyle. Usually results from excessive internal rotation and varus stress resulting in increased tension on the lateral capsular ligament of the knee joint. In the majority of cases a Segond avulsion fracture is associated with detachment of the capsular portion of the lateral collateral ligament and tears of the anterior cruciate ligament. Additional injury to menisci and other supporting ligaments may occur
In 1879 Paul Segond described this fracture during cadaveric experiments as a cortical avulsion of the tibia at the site of insertion of the middle third of the lateral capsular ligament in 17 out of 38 knees. In 1936 Henry Milch first reported the avulsion fracture on radiographs of 3 acutely injured knees
It’s never Gerdy’s tubercle that gives way, but the portion of bone immediately behind it…the lesion is pathognomonic of torsion of the knee in internal rotation and slight flexion of the lower leg and is associated with rupture of the anterior cruciate ligament
Segond 1879
- Paul Ferdinand Segond (1851 – 1912) was a French Orthopaedic Surgeon.
- Segond P. Recherches cliniques et expérimentales sur les épanchements sanguins du genou par entorse. Progrès Médical 1879; 16: 297–299, 319–321, 340–341
Shepherd fracture (1882)
Sherpherd fracture is a posterior talar process fracture with injury to the lateral tubercle caused by inversion or extreme equinus. Otherwise known as fracture of the lateral tubercle of the posterior process of the talus.
- Francis John Shepherd (1851 – 1929) British/Canadian general surgeon and anatomist.
- Shepherd FJ. A Hitherto Undescribed Fracture of the Astragalus (talus). J Anat Physiol. 1882; 17(1): 79–81
Tillaux-Chaput fracture (1876, 1907)

The Tillaux fracture is a fracture of the anterolateral tibial epiphysis commonly seen in adolescents (Salter-Harris III tibial fracture). Tillaux first described from experiments on cadavers in 1876. Chaput was the first to demonstrate a roentgenogram of a fracture in 1907 (*Tillaux-Chaput fracture)
- Paul Jules Tillaux (1834 – 1904) French Surgeon.
- Tillaux PJ. Recherches expérimentales et cliniques sur le mécanisme de la production des luxations coxo-fémorales en arrière. 1876
- Victor Alexandre Henri Chaput (1857 – 1919) French Surgeon.
- Chaput H. Les fractures malléolaires du cou-de-pied et les accidents du travail. [Malleolar instep fractures and occupational injuries] Paris, Masson. 1907
Wagstaffe-Le Fort Fracture (1875, 1886)

Wagstaffe-Le Fort Fracture is a vertical avulsion fracture of the anteromedial aspect of the distal fibula due to avulsion of the anterior tibiofibular ligament attachment (ATFL). [aka Le Fort Ankle Fracture]
- William Warwick Wagstaffe (Sr) (1843-1910) English General surgeon
- Wagstaffe W. An unusual form of fracture of the fibula. St Thomas Hosp Rep. 1875; 6: 43-49
- Léon Clément Le Fort (1829–1893) French surgeon
- Le Fort LC. Note sur une variété non decrite de fracture verticale de la malleole externe par arrachement. [Note on an undescribed variety of vertical fracture of the lateral malleolus by avulsion.] Bull Gen Ther. 1886; 110:193-199
References
- Hunter TB, Peltier LF, Lund PJ. Radiologic history exhibit. Musculoskeletal eponyms: who are those guys? RadioGraphics 2000; 20: 819-36.

eponymythology
myths behind the history
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |